Chapter 14 Cerebellar Tumors in Adults
Many lesions affect the posterior fossa, and the cerebellum in particular. Some tumors, such as brain stem gliomas, cerebellar pontine angle tumors, fourth ventricle tumors, and pineal area tumors extend into the cerebellum from surrounding areas. Metastatic lesions to the cerebellum are also common. However, tumors intrinsic to the cerebellum are less frequent. Primary cerebellar tumors represent only 3.5% of all primary brain and central nervous system (CNS) tumors.1 In children, infratentorial lesions are more prevalent, comprising 16.6% of CNS tumors, while only 6% of primary CNS tumors are found in the cerebellum of adults.1 In this chapter, we will focus only on intrinsic cerebellar tumors.
Clinical Presentation, Diagnosis, and Preoperative Management
Patients with a cerebellar lesion often present with a headache and signs of cerebellar dysfunction. Clinical signs of these deficits are detected by the presence of dysmetria in finger-to-nose or heel-to-shin testing, and dysdiadochokinesis demonstrated by testing of rapid alternating movements. Patients may also present with ataxic tremor, dysarthria, postural instability, or gait disturbances. The cerebellum demonstrates functional localization; cerebellar signs often correlate with the location of the cerebellar lesion.2 The deep cerebellar nuclei have specific deficits when damaged. The midline fastigial nuclei play a role in postural ataxia, whereas globus, embolliform, and dentate nuclei are important for limb ataxia. Injury to the dentate nuclei can lead to dysarthria and mutism in some patients. Midline lesions, affecting the cerebellar vermis and midline cerebellar nuclei, are more likely to demonstrate truncal instability. Lesions involving the cerebellar hemispheres are more likely to show limb ataxias and associated dysmetria.
Patients with a cerebellar mass may also present with symptoms related to compression. Depending on tumor location, large cerebellar tumors can cause compression of the brain stem, which can cause obstruction of the fourth ventricle and various cranial nerve signs, depending on tumor location. Patients may present with hydrocephalus and increased intracranial pressure. Accordingly, headache, nausea, and vomiting are common presenting symptoms for patients with cerebellar tumors.3,4 When a patient presents with signs and symptoms of obstructive hydrocephalus, such as lethargy or coma, an emergent externalized ventricular catheter should be placed prior to surgical planning. In patients with long-standing ventriculomegaly and minimal clinical symptoms, intravenous steroids may alleviate symptoms and obviate the need for an externalized ventricular catheter.
In adult patients that present with a suspected cerebellar mass, an appropriate work-up should be done to obtain as much information as possible prior to surgery. Neuroimaging typically involves computed tomography (CT) and magnetic resonance imaging (MRI). CT scans have the advantage that they can be done rapidly, and thus help determine immediate treatment upon initial presentation of the patient. MRI gives better visualization of the posterior fossa, and is thus the imaging modality of choice for patients with a suspected cerebellar lesion. The appearance of the lesion in the MRI sequences can help narrow the differential diagnosis of the lesion. Cerebellar tumors can be identified as solid or cystic. Solid components of tumors can be evaluated with T1 and T2 MRI sequences. Most solid components are isointense to gray matter on T1 and T2; however, tumors such as pilocytic astrocytomas can appear isointense to cerebrospinal fluid (CSF) on T2.5,6 For tumors that are highly vascular, such as hemangioblastomas, diffusion-weighted imaging (DWI) will show low signal, and apparent diffusion coefficient (ADC) will show increased signal within the solid vascular portion of the tumor. This imaging pattern contrasts with tumors that are highly cellular, such as medulloblastoma, that will have high DWI and low ADC signal.6 Tumors that have abnormal vessels, such as in Lhermitte-Duclos, or tumors with evidence of prior hemorrhage, will benefit from susceptibility-weighted imaging (SWI) sequences, which are sensitive to venous blood and hemorrhage.7 Cystic portions of tumors are generally hypointense on T1 and hyperintense on T2 due to the liquid component; fluid attenuation inversion recovery (FLAIR) sequences can be helpful in tumors such as hemangioblastomas where the cystic component is different from CSF.6 Tumors with a large percentage of fat-containing substance, such as in cerebellar liponeurocytomas, can be identified by hyperintense streaks on T1, and fat suppression sequences can aid in their diagnosis.8 The pattern of contrast enhancement after the administration of gadolinium is also useful, as some cerebellar tumors enhance strongly and homogeneously, whereas others show heterogeneous enhancement patterns.
Patients, especially adults, with a cerebellar mass should also receive screening scans to evaluate for possible metastatic disease to the cerebellum. Such a workup should include imaging of the chest (via chest x-ray and/or CT scan of the chest) and also CT of the abdomen and pelvis. The treatment of metastatic lesions to the cerebellum is often dictated by a number of factors, including the identity of the tumor of origin, the size, location, and number of metastases. Please refer to the subsequent chapter on metastatic lesions for further details.
Intrinsic Cerebellar Tumors in Adults
Cerebellar Astrocytomas
Gliomas represent 36% of all primary brain and CNS tumors; of these, 3% are located in the cerebellum.1 Gliomas of the cerebellum are frequently astrocytomas. The most common is the pilocytic astrocytoma, which represents between 70% to 90% of cerebellar astrocytomas.3,9 Pilocytic astrocytomas are low-grade, World Health Organization (WHO) classification grade I tumors that represent 5% to 6% of all gliomas.10 In children they are the most common glioma, of which 67% occur in the cerebellum. In adults, the location of pilocytic astrocytomas is evenly distributed between supra- and infra-tentorial lesions.9,11
Cerebellar pilocytic astrocytomas demonstrate consistent imaging features. These tumors are found equally in the cerebellar vermis or hemispheres. They appear as well-circumscribed, unencapsulated lesions that often have cyst formation and a solid mural nodule. The solid component of the tumor is often isointense to CSF on T2 MRI and shows strong contrast enhancement.5 Tumor necrosis is not evident in histopathologic evaluation. Classically, pilocytic astrocytomas show regions with compact bipolar cells that alternate with microcystic, loosely organized regions. Eosinophilic granular bodies and Rosenthal fibers are commonly present.
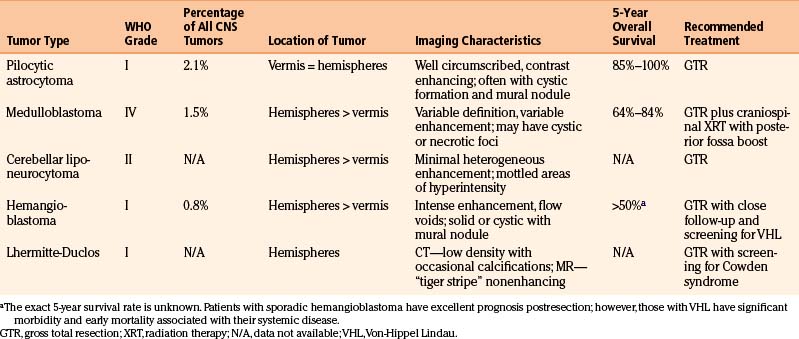
These tumors generally have a good prognosis after surgical resection with an 85% to 100% 5-year survival rate.1,9,10 The favorable prognosis in these patients has been attributed to the low-grade nature of cerebellar pilocytic astrocytomas and the ability to achieve a gross total resection. It has been documented that surgeons tend to overestimate the degree of tumor resection.12 As most tumor recurrence is related to residual tumor,12,13 it is recommended that within 48 to 72 hours after surgery an MRI, with and without gadolinium, be obtained to determine if gross total resection has occurred. Rarely, malignant transformation of pilocytic astrocytomas can occur.14 Adjuvant therapy, either radiation or chemotherapy, is not indicated for patients with cerebellar pilocytic astrocytomas, as gross total resection alone yields excellent prognosis.9,11 The characteristics of cerebellar astrocytomas are summarized and compared to other intrinsic cerebellar tumors in Table 14-1.
Not all astrocytomas found in the cerebellum are low-grade pilocytic astrocytomas. The pilomyxoid astrocytoma (PMA) is an astrocytoma that shows similarities to the pilocytic astrocytoma, but histopathology confirms it lacks Rosenthal fibers, has a mucoid matrix, and shows an angiocentric arrangement of tumor cells, making it a distinct entity. Additionally, PMA is more aggressive, defined as WHO grade II, and often shows CSF dissemination at presentation.10,15 The PMA is found most frequently in children; however, cases have been reported in adults, and PMAs have been detected in the cerebellum.16,17 It has been demonstrated that up to 6% of astrocytomas presenting in the cerebellum are WHO grade III, and 17% exhibit the more malignant features of glioblastoma multiforme.3 Radiographic features of these tumors include heterogeneous contrast enhancement and significant edema; leptomeningeal spread is common.18 Because of the infiltrating nature, or the involvement of deep-seated tissues, these tumors are not cured by surgery and recur with higher frequency. For this subset of high-grade cerebellar astrocytomas, additional treatment modalities such as radiation, chemotherapy,19,20 and/or radiosurgery have been performed.21,22
Medulloblastomas
Embryonal tumors, including medulloblastoma, represent 1.5% of primary CNS tumors.1 Medulloblastomas are malignant WHO grade IV tumors of the cerebellum, of which 70% occur in children under the age of 16 years. They are fairly common in children, representing 20% to 30% of all intracranial neoplasms in the pediatric sector, whereas in adults there is an incidence of approximately 0.5 per million.23,24 In adults, medulloblastomas are rarely seen beyond the fifth decade of life. Eighty percent occur in patients aged 21 to 40 years.10 Most childhood medulloblastomas are found in the vermis. With increasing age, there is a progressive involvement of the cerebellar hemispheres, thus the majority of adult medulloblastomas are hemispheric. Additionally, there are radiographic differences in the appearance of childhood and adult medulloblastomas. In children, the classic radiographic appearance is that of a well-defined homogenous tumor that shows marked contrast enhancement and is without cystic or necrotic degeneration. In comparison, adult medulloblastomas are more variable in appearance (see case report 1). They are not as well defined, the degree of contrast enhancement varies, and there are often small cystic or necrotic foci.25,26 Adult patients are also more likely to exhibit the desmoplastic nodular subtype of histopathology. Nodular, reticular free regions of neuronal maturation surrounded by densely packed proliferative cells that produce an intercellular reticulin fiber network characterizes this subtype. It is thought that this desmoplastic subtype may contribute to some of the variety seen on radiographic imaging, but it is unclear whether this subtype affects prognosis.26–28
Despite the differences in childhood and adult medulloblastoma, the recommended treatment regimen is similar. Standard treatment involves gross total resection followed by craniospinal irradiation. Given this treatment, the 5-year overall survival for adult medulloblastomas is 64% to 84%.23,29–31 Many factors influence the outcome of adult patients with medulloblastoma. Approximately 18% to 33% of patients have metastatic disease at presentation including spinal cord, CSF, and extraneural metastases. Metastasis has been shown to be a poor prognostic indicator, as has involvement of the brain stem, involvement of the floor of the fourth ventricle, radiation dose less than 50 Gy, and large-cell variant histopathologic subtype.23,29,32,33 In contrast, patient age less than 20, gross total resection of tumor, and completion of radiation treatment within 48 days are known to be positive prognostic indicators.23,30
Recent studies have explored the role of adjuvant chemotherapy for patients with adult medulloblastoma. The benefit of chemotherapy is still unclear in the adult medulloblastoma population so there are no universal guidelines for administration of chemotherapy. Gross total resection and radiation are the most important factors in preventing recurrence, and primary adjuvant chemotherapy has not been shown to have a significant association with survival.33,34 However, for high-risk patients, it appears that chemotherapy may delay the risk of recurrence by approximately 3 years, and thus, there may be a role for chemotherapy in a subpopulation of adult patients with medulloblastoma.32,35 For patients with widely metastatic medulloblastoma who have failed multiple treatment options, new chemotherapy techniques that target tumor-specific mutations show promise as future treatment modalities.36
Case Report 1: Medulloblastoma
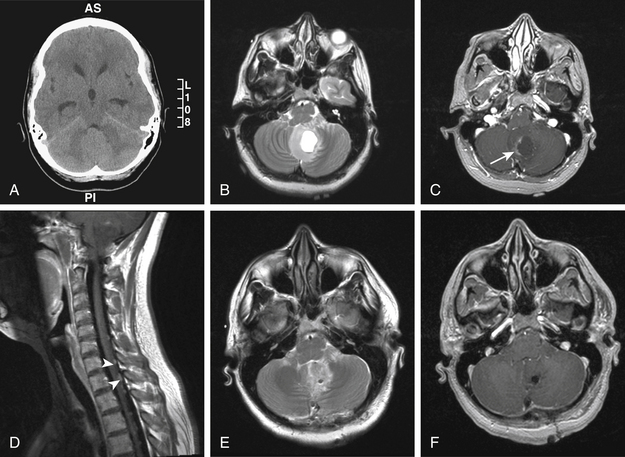
A 22-year-old female, without a significant past medical history, presented to the emergency department with 2 weeks of occipital headache and blurry vision. Ophthalmology evaluation revealed papilledema and dysconjugate gaze. On examination she was sleepy, but arousable, and able to follow simple commands. Head CT revealed a cerebellar lesion with mass effect causing some effacement of the fourth ventricle and hydrocephalus (Fig. 14-1A).
Cerebellar Liponeurocytoma
Cerebellar liponeurocytoma is a rare cerebellar neoplasm found primarily in adults.10 It has previously been named in the literature as lipomatous medulloblastoma, neurolipocytoma, medullocytoma, and lipomatous glioneurocytoma. The now widely accepted name is cerebellar liponeurocytoma. Initially, this entity was thought to hold similarities to medulloblastomas, but the cerebellar liponeurocytoma is distinct. It is found primarily in adults and typically presents in the fifth or sixth decade, which is substantially older than the age of presentation for medulloblastomas. Additionally, cerebellar liponeurocytomas have a low proliferative index, and therefore a favorable prognosis. Although they do not exhibit malignant transformation, they have a recurrence rate of approximately 50%, with a mean time to recurrence of approximately 10 years.37,38 Because of the propensity for recurrence, cerebellar liponeurocytomas are designated as WHO grade II.10
On neuroimaging, cerebellar liponeurocytomas can be difficult to distinguish from other more common cerebellar tumors. They are prevalent in the cerebellar hemispheres as compared to the vermis. MRI T1 imaging usually demonstrates a hypointense lesion with mottled or streaked areas of hyperintensities that correspond to adipose containing areas. These lesions are usually associated with a minimal amount of heterogeneous enhancement, and minimal associated edema.8,10 The main criterion distinguishing this tumor type from others in the cerebellum is the presence of intratumoral areas of fat. Histologically, this is represented by cells showing advanced neuronal differentiation and areas of focal accumulation of mature lipidized tumor.
Similarly to other cerebellar neoplasms, treatment is gross total resection. Cerebellar liponeurocytomas have a tendency for exophytic growth into CSF spaces and gross total resection is not always obtainable. Yet, the role of adjuvant radiotherapy or chemotherapy has not been established. Some authors believe that due to the nature of these tumors to recur, it is feasible to consider adjuvant radiotherapy to the posterior cranial fossa immediately after the initial surgery.39 Yet others suggest that radiation therapy is best reserved for evidence of recurrence.38 Regardless, most are in agreement that due to the nonmalignant nature of these tumors, aggressive radiotherapy, as is standard for medulloblastomas, is not necessary for cerebellar liponeurocytomas.
Hemangioblastomas
Hemangioblastomas represent about 1% of all intracranial tumors,1 but about 8% of posterior fossa tumors in adults. They are slow-growing, highly vascular tumors that are classified as WHO grade I.10 Hemangioblastomas occur most frequently in the cerebellum; however, they can also be found in the brain stem or spinal cord.
Cerebellar hemangioblastomas are distinct on neuroimaging. Classically, they can be solid, solid with cystic component, or cystic with nodule (see case report 2). They are found more commonly in cerebellar hemispheres as compared to the vermis.40,41 Due to the highly vascular nature of these tumors, flow voids are usually present. In addition, these tumors are heterogeneous in T2, and show intense contrast enhancement.42 Angiography is useful to evaluate the tumor feeding vessels prior to surgical intervention.
Approximately 30% of patients with cerebellar hemangioblastomas have the multisystem cancer syndrome Von-Hippel Lindau (VHL). Patients with VHL develop numerous visceral lesions including renal cell carcinoma, pancreatic islet cell tumors, pheochromocytoma, and papillary cystoadenomas of the epididymis and broad ligament. CNS manifestations include endolymphatic sac tumors and multiple hemangioblastomas. The hemangioblastomas typically occur in the retina, brain stem, cerebellum, spinal cord, and nerve roots. Patients with VHL tend to be younger, and have multiple hemangioblastomas at presentation.41,43–45
Sporadic, compared to VHL-associated cerebellar hemangioblastomas, are not significantly different in location within the cerebellum, solid versus cystic type, or surgical outcomes. Treatment of cerebellar hemangioblastoma involves gross total resection and typically has a favorable prognosis. However, VHL patients have significant morbidity related to their systemic disease, and are more likely to develop additional hemangioblastomas, with an average of one every 2.1 years.43 Thus, the subgroup of patients with VHL must be recognized. Any patient with a cerebellar hemangioblastoma should undergo appropriate screening for VHL. At a minimum, this should include neuroimaging of the neuraxis to look for additional hemangioblastomas. Because patients with VHL often have multiple hemangioblastomas, it is important to have thresholds for treatment of these lesions. Tumors that need resection are generally those that are, or will become, symptomatic. The strongest predictors of symptomatic progression are tumor/cyst growth greater than 112 mm3 per month and tumor/cyst size greater than 69 mm.3,41 Hemangioblastomas in VHL can be asymptomatic, and these patients require long-term follow-up with imaging every 6 to 12 months.
Adjuvant radiotherapy has been considered in some cases of hemangioblastomas. Given that gross total resection gives a favorable prognosis, cases of stereotactic radiosurgery or fractionated external beam radiotherapy are generally preserved for those patients with subtotal resection or tumor recurrence.46 For patients receiving adjuvant stereotactic radiosurgery, better progression-free survival has been associated with smaller tumor volumes, solid tumor type, and margin dose of 15 Gy or more.47
Case Report 2: Hemangioblastoma
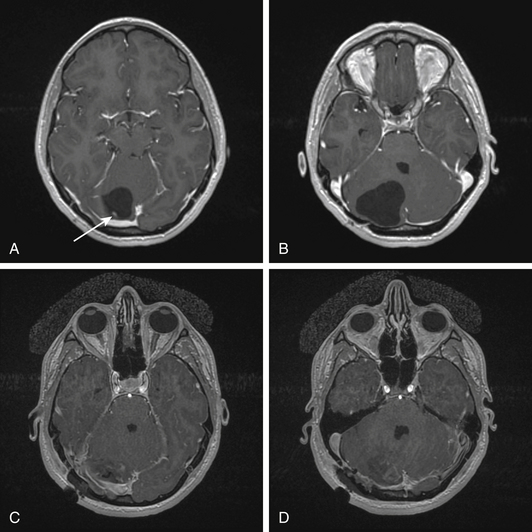
Imaging revealed an enhancing mural nodule near the torcula (Fig. 14-2A, arrow) within a large cystic lesion (B). Imaging of the neuraxis did not reveal any additional lesions.
< div class='tao-gold-member'>
Related posts:
 Prolactinomas
Prolactinomas
 Surgical Management of Cerebellar Stroke–Hemorrhage and Infarction
Surgical Management of Cerebellar Stroke–Hemorrhage and Infarction
 Surgical Management of Tumors of the Foramen Magnum
Surgical Management of Tumors of the Foramen Magnum
 Contemporary Dorsal Rhizotomy Surgery for the Treatment of Spasticity in Childhood
Contemporary Dorsal Rhizotomy Surgery for the Treatment of Spasticity in Childhood
 Role of Gamma Knife Radiosurgery in the Management of Arteriovenous Malformations
Role of Gamma Knife Radiosurgery in the Management of Arteriovenous Malformations
 Arachnoid, Suprasellar, and Rathke’s Cleft Cysts
Arachnoid, Suprasellar, and Rathke’s Cleft Cysts
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


