56 Cerebral Venous Thrombosis
When venous drainage of the brain is compromised, arterial flow creates back-pressure into tissue capillaries causing capillary congestion, interstitial edema, decreased tissue perfusion, and ultimately ischemia. Eventually capillary rupture causes hematoma formation. This process of cerebral venous congestion followed by infarction (not conforming to strict arterial territories) and hemorrhage is the hallmark of cerebral sinus thrombosis. The causes of cerebral venous thrombosis vary (Box 56-1), but many relate to transient or permanent hypercoagulable states, with dehydration acting as a common precipitating event. A thorough investigation for such etiologies is crucial to directing long-term treatment and anticipating potential comorbidities.
Anatomy
The dura is formed of two layers, one abutting the inner calvarium and the other forming the outer meningeal covering. These layers separate in the midsagittal and transverse planes, forming dural venous sinuses ultimately draining into the jugular veins. A single superior sagittal sinus joins the often asymmetric but paired transverse sinus at the confluence of sinuses or torcular herophili (Fig. 56-1). The transverse sinuses run laterally from the occipital bone to the middle cerebral fossa along the tentorium cerebelli. The right is often larger and is continuous with the superior sagittal sinus whereas the left curves out laterally as an extension of the single midline straight sinus. The straight sinus runs downward from near the splenium of the corpus callosum to the occipital protuberance. The sigmoid sinus curves down toward the skull base from the transverse sinus and joins the inferior petrosal sinus at the jugular foramen to form the jugular vein.
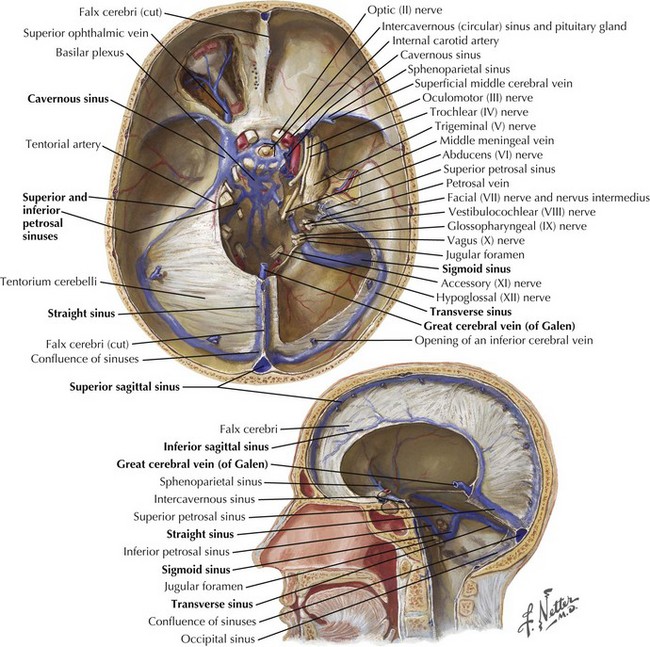
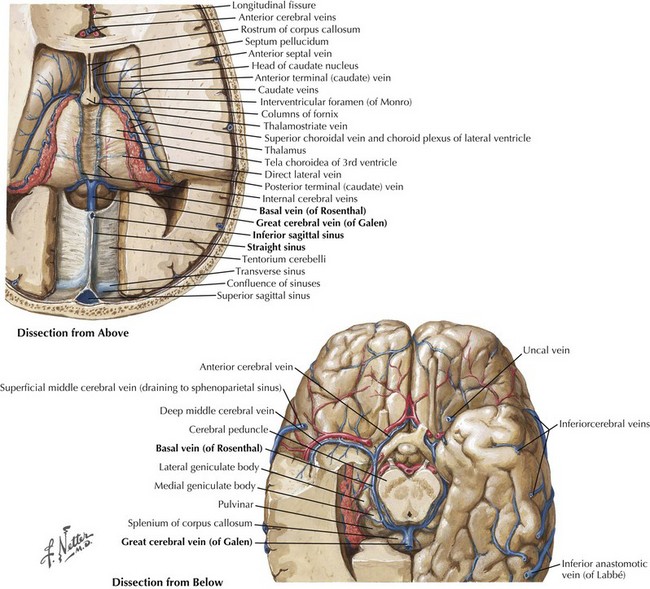
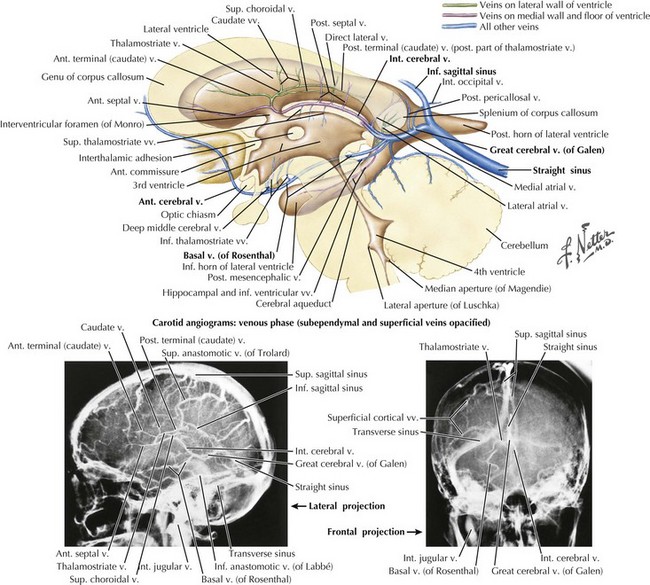
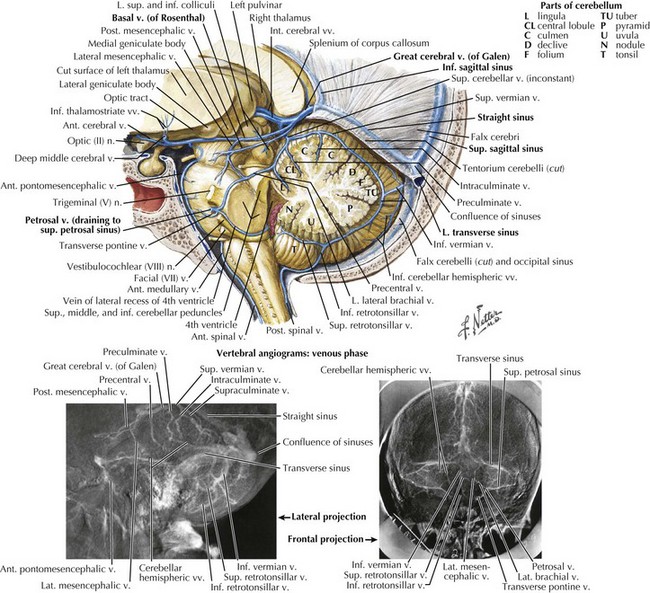
The straight sinus (Figs. 56-1 through 56-4) is formed by the splayed falx layered over the cerebellar tentorium. The inferior sagittal sinus runs in the fold of the lower arch of the falx cerebri and joins the cerebral vein of Galen in the proximity of the posterior horns of the lateral ventricles to form the straight sinus. The superior and inferior sagittal sinuses provide drainage for the cerebral hemispheres.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


