Anticoagulant therapy is primarily utilized for deep venous thrombosis prophylaxis in patients with acute ischemic stroke.
Anticoagulant therapy has a potential role in ischemic stroke prevention if there is a documented cardioembolic source, in hypercoagulable conditions, in cerebral sinovenous thrombosis, and perhaps in cerebrovascular dissection.
There is a growing literature on interventional therapy in acute ischemic stroke, but intravenous recombinant tissue plasminogen activator, initiated within 3 hours of presentation, remains the only FDA-approved medication.
Endovascular techniques are becoming increasingly utilized for cerebrovascular anomalies such as aneurysms and arteriovenous malformations.
Cerebrovascular disease includes both primary ischemic stroke (large artery thrombotic, e.g., lacunar-type, embolic, and hemodynamic, small artery thrombotic, e.g., watershed-type, vasculitis-induced infarction, vascular dissection-induced infarction, and sinovenous thrombotic infarction) and hemorrhagic stroke (primary intracerebral hemorrhage [ICH] and subarachnoid hemorrhage [SAH]). In addition, one can see hemorrhagic transformation of an initially ischemic stroke and this is one of the major concerns with the use of either recombinant tissue plasminogen activator (rt-PA) or anticoagulant therapy in acute ischemic stroke. Stroke, which is a generic term for damage to the central nervous system (CNS) on a vascular basis, is a common presentation in the emergency department. Most strokes are readily diagnosed on the basis of a sudden constellation of neurologic deficits in a patient with well-recognized risk factors for cerebrovascular disease.
Iatrogenic, i.e., related to antithrombotic therapy
Embolic
Septic aneurysm
Cardiogenic
Aortic arch atheromata
Artery-to-artery
Arteritis
It is estimated that there are roughly 750,000 first or recurrent strokes in the United States per year. This translates to approximately 250 stroke patients per 100,000 per year. The frequency of stroke type varies depending on the patient population. For example, a retirement community is more likely to have patients of advanced age with a relatively high incidence of atherosclerotic disease seen in tandem with hypertension, diabetes mellitus, hyperlipidemia, and coronary artery disease. A hospital in a community of young and middle-aged people will tend to see more esoteric causes of stroke, such as lupus vasculitis, hypercoagulable states, sinovenous occlusive disease as a complication of pregnancy, stroke related to oral contraceptive use, paradoxical cerebral embolism related to an atrial septal defect, and vascular dissection (which often has trauma as an initiating factor).
Roughly 80% to 85% of all stroke is primary ischemic and 15% to 20% is primary hemorrhagic. Of the ischemic strokes, approximately 50% to 60% are large artery thrombotic; 20% are small artery thrombotic (lacunar-type); 15% to 20% are cardiogenic or artery-to-artery emboli; and 5% to 10% are less common etiologies such as vasculitis, dissection, septic or nonseptic emboli, or sinovenous occlusive disease. Approximately 5% to 6% of all strokes are SAH, usually related to rupture of a cerebral aneurysm or bleeding from an arteriovenous malformation (AVM), whereas 10% to 15 % are primary ICH. The major stroke etiologies are listed in Table 7.1.
▪SPECIAL CLINICAL POINT: Determination of stroke mechanism is important since it has a direct impact on management.
IDENTIFICATION OF THE STROKE-PRONE INDIVIDUAL
It has become increasingly important to identify patients with risk factors for stroke (Table 7.2) because there is an increasing armamentarium of potential therapies to reduce stroke risk. Conversely, the interventional therapies for acute stroke remain quite limited. Transient ischemic attack (TIA) is a warning of ischemic stroke, and it can precede up to 15% of all stroke. It represents an opportunity to identify a patient who is at particular risk for ischemic stroke in an effort to institute effective prevention. Prior stroke and TIA are major identifiers of stroke-prone individuals. In a study of patients with TIA presenting to the emergency room (ER), 10.5% of patients returned to the ER within 90 days with a stroke and half of these events occurred within 2 days of the TIA. The risk of recurrent stroke is very much reflective of the stroke mechanism and how aggressively risk factors are managed. The risk of recurrent stroke is 10% to 12% per year, but this can be impacted by optimal blood pressure management, aggressive control of hyperlipidemia, smoking cessation, and an effective diet and exercise programs.
TABLE 7.2 Risk Factors for Stroke
Major Risk Factors
Minor Risk Factors
Age
Hypercholesterolemia
Sex
Oral contraceptives
Race
Migraine
Genetic predisposition
Obesity
TIA/prior stroke
Physical inactivity
Hypertension
Mitral valve prolapse
Acute myocardial infarction with thrombus
Patent foramen ovale
Bacterial endocarditis
Diabetes mellitus
Marantic endocarditis
Cigarette smoking
Sick sinus syndrome
Valvular heart disease
Aortic arch atheromatia
Atrial fibrillation
Polycythemia
Dilated cardiomyopathy
Bleeding diathesis
Peripheral vascular disease
Sympathomimetic agents including cocaine
Sickle cell anemia
Hyperhomocysteinemia
Hypercoagulable state
Thrombocytosis
▪SPECIAL CLINICAL POINT: A transient ischemic attack (TIA), when properly recognized, represents an important opportunity to effectively intervene before the stroke occurs.
The risk of stroke increases exponentially with age, and the risk is higher for males. African Americans appear to be more susceptible to stroke than Caucasians. For example, intracranial stenosis, which can account for up to 10% of all ischemic stroke, tends to be more prevalent in African Americans, Hispanics, and Orientals. In contrast to African Americans, Caucasians appear to be more susceptible to symptomatic extracranial carotid stenosis. Naturally, the presence of contributing factors to atherosclerosis, such as hypertension, hyperlipidemia, diabetes mellitus, familial predisposition, and smoking consumption impact on stroke type and frequency. In addition, cumulative cardiac factors can play a major role in predisposition to cardioembolic stroke. An example of this is atrial fibrillation. Lone atrial fibrillation (AF) in a person under 60 years of age is not a significant risk factor for stroke. However, the coexistence of AF with such factors as valvular heart disease, ischemic cardiomyopathy, hypertension, or prior embolic events translates into a much greater risk of cardioembolic stroke.
▪SPECIAL CLINICAL POINT: So-called “lone atrial fibrillation” (atrial fibrillation in a patient less than 60 years of age with a structurally normal heart and no risk factors for stroke) is associated with a stroke risk that is essentially that of an age-matched individual without atrial fibrillation.
CLINICAL EVALUATION
The history is obviously a vital aspect of the diagnostic assessment of patients presenting with stroke-like symptoms. The most common presentation for stroke is the sudden onset of focal neurologic deficit(s) in a patient with risk factors for stroke, with increasing age being a particularly important indicator. The term “stroke in the young” promotes recognition of patients 45 years of age or younger who do not have a readily identifiable predisposing factor. In such circumstances, more esoteric explanations for the stroke should be sought such as lupus vasculitis, primary CNS vasculitis, drug-induced vascular compromise, moyamoya disease, sickle cell disease, paradoxical cerebral embolus, meningovascular syphilis, and sinovenous thrombosis and hypercoagulable conditions.
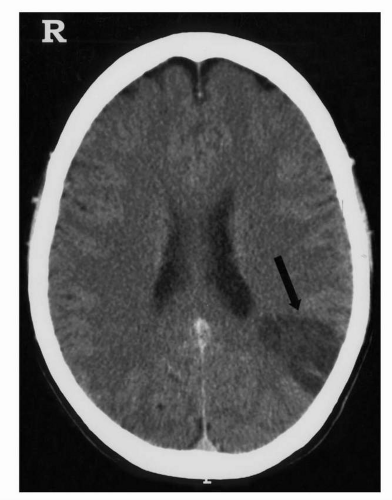
Proper recognition of stroke has become even more important with the advent of thrombolytic therapy, specifically rt-PA, which must be administered intravenously within 3 hours of symptom onset. This is the only agent presently available for acute ischemic stroke. To be eligible for rt-PA, patients need to be assessed, have certain blood tests performed, and have a noncontrast computed tomography (CT) brain scan performed within the 3-hour time window before the agent can be infused (Fig. 7.1). The initial history must place emphasis on determination of the exact time that the symptoms began and pertinent past medical factors such as prior bleeding, recent surgery, or trauma that might enhance the bleeding complication rate with rt- PA. It is important to note that patients who wake up with their deficits have to have the onset assigned to the time that they were last neurologically unaffected. For example, if they woke up with a stroke at 6 AM and were last awake at 11 PM the evening before, then it has to be assumed that the stroke occurred just after 11 PM. However, if the patient had gone to the bathroom at 5 AM, and they were perfectly fine, and then went back to bed and awakened at 6 AM with the stroke, it can be assumed that the stroke occurred just after 5 AM. This would translate into a 2-hour window of opportunity for treatment with rt-PA (i.e., 6 to 8 AM).
FIGURE 7.1 Noncontrast CT brain scan which demonstrates an infarct (arrow) that has already evolved. This would mitigate against the use of recombinant tissue plasminogen activator (rt-PA) in such a circumstance, as there is already hypodensity implying already infarcted tissue and the onset would be presumably well beyond 3 hours based on this scan. The distribution of the infarct is the left watershed region between the middle cerebral artery and posterior cerebral artery that can imply a hemodynamic mechanism.
The use of rt-PA mandates a more standardized approach to the neurologic evaluation for a patient with acute stroke, and this, fortunately, has been extended to most stroke patients even if they are not candidates for the medication. For example, it is important to obtain a CT brain scan at the time of presentation to readily distinguish a primary ischemic stroke from a primary hemorrhagic stroke. Generally, contrast is not necessary unless there are clinical concerns that the patient might have a tumor or abscess instead of a stroke. It is important to recognize that the CT brain scan has a sensitivity of 90% to 95% for the detection of SAH. Therefore, clinical suspicion for SAH, even with a negative CT brain scan, mandates the performance of a lumbar puncture unless there are contraindications. In addition to the CT brain scan, routine immediate blood work includes a complete blood count (CBC), platelet count, metabolic profile, prothrombin time (PT)/international normalization ratio (INR), and partial thromboplastin time (PTT).
Furthermore, a more standardized approach to the neurologic examination has been adopted to quantitate the degree of deficit in a more objective and reproducible pattern. This is especially pertinent for patients who are potentially eligible for rt-PA. The National Institutes of Health (NIH) Stroke Scale is used to provide such standardization. This is in recognition that rt-PA should only be considered for patients with a significant neurologic deficit at the time of presentation; rt-PA should not be used if the patient is rapidly improving. There are potentially greater risks of complications of rt-PA and a reduced chance of benefit from therapy when the patient has a high score on their NIH Stroke Scale. This scale correlates with severity of neurologic deficit.
TABLE 7.3 Features of Thrombotic Versus Embolic Stroke
Branch occlusion pattern on brain scan or angiography
Other evidence of large vessel disease
Embolic involvement of other organs
Severe deficit at onset followed by rapid resolution
▪ SPECIAL CLINICAL POINT: The greater the time from the onset of stroke, the greater the evolution of an infarction pattern by CT brain scan, the greater the degree of neurologic deficit, the poorer the control of blood pressure, the higher the admission blood glucose, as well as possibly the greater the age of the patient, the greater the likelihood of hemorrhagic transformation with rt-PA.
There are certain presentation characteristics that help identify the stroke mechanism (Table 7.3). For example, cerebral embolus, as opposed to thrombosis, tends to occur with maximum neurologic deficit at onset. There can be syncope and/or seizure at the time of presentation due to the sudden cessation of the circulation. Involvement of different vascular territories and a documented source of cardiogenic embolus are other features strongly supportive of an embolic mechanism. Conversely, thrombotic stroke tends to occur in a stepwise fashion, is reported to be more commonly associated with premonitory TIA, and is associated with risk factors for atherosclerosis or lipohyalinosis. Embolic events tend to result in cerebral artery branch occlusions.
DIAGNOSTIC EVALUATION
Table 7.4 outlines the first-, second-, and thirdtier diagnostic studies that are part of the stroke evaluation. The first tier represents the routine studies that are performed on any patient presenting with symptoms of TIA or stroke. Obviously the clinical picture will affect the choice and speed with which the study is performed. For example, a patient presenting with new-onset TIA should undergo immediate evaluation of the potential ischemic mechanism in an effort to intervene before a stroke occurs.
TABLE 7.4 Hierarchy of Studies in Acute Ischemic Stroke
First tier
Noncontrast CT brain scan
CBC, platelet count, PT, INR, and PTT
Serum chemistry profile EKG
Fasting lipid profile
Second tier (if clinically indicated)
Contrast-enhanced CT brain scan
MRI brain scan
Carotid/vertebral duplex scan
Transcranial Doppler ultrasonography
Transthoracic echocardiogram
Holter monitor
Magnetic resonance angiography and/or venography vs. CT angiography
Blood cultures
ESR
Lumbar puncture
Urine drug screen
Third tier (if clinically indicated)
Cardiac stress test
Transesophageal echocardiogram
Cerebral arteriography
HIV test
Syphilis testing
Sickle cell prep
Bleeding time
Platelet function studies
Special clotting studies
Fasting homocysteine level
C-reactive protein
Proteins C and S levels
Proteins C and S levels
Antiphospholipid antibodies
Genetic testing for MELAS(mitochondrial myopathy, lactic acidosis, and stroke-like episodes), Fabry disease, CADASIL (cerebral autosomal-dominant arteriopathy with subcortical strokes and leukoencephalopathy), etc.
The same is true for relatively minor stroke associated with resolution of signs and symptoms within days to weeks. However, there is usually little to offer the patient who is moribund from a stroke.
▪SPECIAL CLINICAL POINT: It is important to determine whether or not particular testing will impact management. This will help avoid unnecessary costs as well as testing that may be associated with risks that are best avoided.
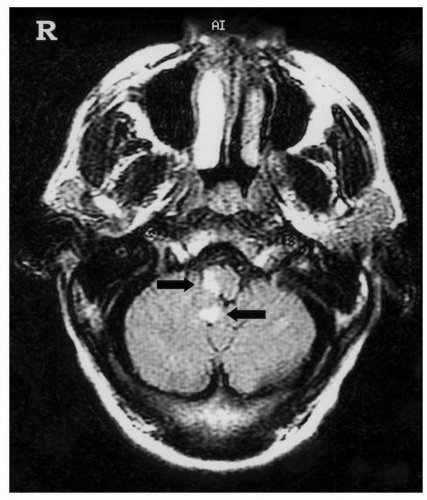
The CT brain scan is often the only neuroimaging study that is necessary for acute stroke evaluation. Contrast is usually not necessary, and this represents a practical and cost-effective approach for most patients. However, there are certain patients in whom a magnetic resonance imaging (MRI) brain scan may provide worthwhile information that may affect patient management —for example, in the patient with an atypical or fluctuating clinical picture with evidence of brainstem or cerebellar involvement an MRI typically provides a much better image of this area and can help to confirm the clinical impression (Fig. 7.2). Other potential advantages of MRI include the greater safety of using contrast-enhanced MRI, as opposed to contrast-enhanced CT scan. In addition, magnetic resonance angiography (MRA) and venography (MRV) have the ability to provide a reasonably accurate view of the extracranial and intracranial circulation, which often provides information complementary to the MRI. CT angiography (CTA) appears to have better definition than MRA in most circumstances. However, CTA requires intravenous infusion of iodine-based contrast. These less-invasive studies vary in quality between institutions and do not yet have the accuracy of the “gold standard” for the evaluation of the cerebral circulation, which remains intra-arterial cerebral arteriography.
FIGURE 7.2 T2-weighted MRI brain scan that demonstrates signal hyperintensity with the anterior arrow pointing to a right brainstem infarct and the posterior arrow showing infarction within the cerebellum.
Diffusion-weighted imaging (DWI) as a component of the MRI brain scan in acute ischemic stroke allows detection of cellular injury and cytotoxic edema (Fig. 7.3). MR perfusion imaging can identify brain tissue that is susceptible to infarction but that is in a potentially salvageable state. Thus, a so-called “perfusion-diffusion mismatch” might be of value in identifying acute ischemic stroke patients who are most likely to respond to rt-PA. However, such an approach requires ready availability of these MRI techniques and immediate reading of images. Any delay associated with obtaining these studies further prolongs the initiation of rt-PA, which limits the usefulness of perfusion-diffusion images. In situations in which there is some difficulty in distinguishing an ischemic stroke from another process, the finding of hypointensity on the apparent diffusion coefficient (ADC) image that correlates with hyperintensity on the DWI, in the same region, supports acute ischemia (see Chapter 4, Fundamentals of Neuroradiology).
Only gold members can continue reading. Log In or Register to continue