Cranio-Cervical Junction Acute Injury
Julia Crim, MD
DIFFERENTIAL DIAGNOSIS
Common
Trauma
Odontoid C2 Fracture
Burst Fracture, C2
Hangman’s C2 Fracture
Jefferson C1 Fracture
Occipital Condyle Fracture
Dissection, Vertebral Artery
Traumatic Disc Herniation
Os Odontoideum
Spinal Cord Injury Without Radiographic Abnormality (SCIWORA)
Nontraumatic Mimics
Pathologic Vertebral Fracture
Craniovertebral Junction Variants
Incomplete Fusion, Posterior Element
Pseudosubluxation C2-3
Torticollis
Less Common
Atlanto-Occipital Dislocation
Atlanto-Axial Rotary Subluxation
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
MR very useful to evaluate for ligament injuries
Coronal STIR rarely performed but useful in this region
Coronal, sagittal reformations essential on CT for full evaluation of injury
CT arteriogram equally accurate and faster than MR arthrogram for vertebral dissection
Time is often of the essence in these patients, who tend to have multiple injuries
Helpful Clues for Common Diagnoses
Odontoid C2 Fracture
Usually low-velocity injury in elderly
Jefferson C1 Fracture
If combined displacement of lateral masses > 6.9 mm, unstable
High likelihood of other fractures: Spine, skull, pelvis, lower extremity
Os Odontoideum
Chronic, nonunited odontoid fracture
Spinal Cord Injury Without Radiographic Abnormality (SCIWORA)
Occurs primarily in children
MR: Injuries to cord, ligaments, intervertebral discs, cartilaginous endplates
2/3 severe cervical injuries in children < 8 years are SCIWORA
Pseudosubluxation C2-3
Children < 10 years old, anterolisthesis may measure up to 4 mm
Helpful Clues for Less Common Diagnoses
Atlanto-Occipital Dislocation
High incidence cord injury
Formerly usually fatal; now often survive to hospital
Image Gallery
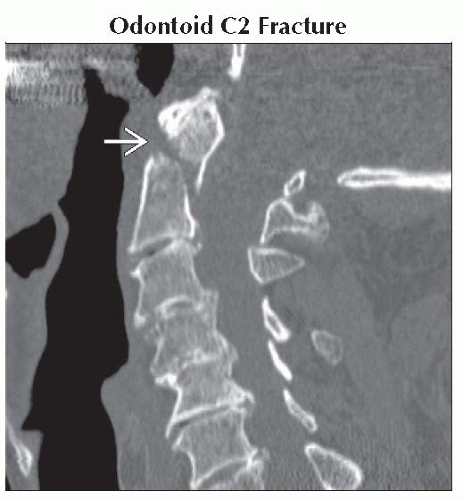 Sagittal NECT shows type 2 dens fracture
 in an osteoporotic patient. Soft tissue swelling is mild. These fractures are commonly subtle on radiographs and best seen on lateral (not odontoid) view. in an osteoporotic patient. Soft tissue swelling is mild. These fractures are commonly subtle on radiographs and best seen on lateral (not odontoid) view.Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|