Chapter 17 Discogenic Pain and Discography for Spinal Injections



History and Background
Discography has become a valuable diagnostic tool since its introduction in the 1940s to diagnose lumbar disc herniation.1–3 Since discography was introduced, computed tomography (CT) and magnetic resonance imaging (MRI) scanning have also added to our knowledge of the lumbar discs; however, because structural abnormalities such as degenerative disc changes, herniations, and annular tears occur in patients asymptomatic of low back pain,4,5 discography is the only direct method to asses if a disc is painful or not. Discography has also been shown to reveal abnormalities in symptomatic patients with normal MRI scans.6,7
Today, discography is used most often to identify painful internally disrupted discs.3 Discography is unique in that it is the only diagnostic technique that directly correlates a patient’s symptoms with disc morphology.4 This is analogous to palpation, which is fundamental to physical diagnosis.5 Tenderness elicited on palpation is analogous to pain provocation on discography.
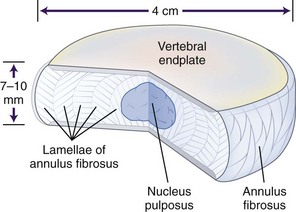
When evaluating a suspected spinal origin of pain, it is critically important to assess the significance of pathological findings on imaging studies and to determine whether those findings correlate with a patient’s symptoms. Discography is distinctive in its ability to make this determination. Discography is used in the lumbar,6–19 thoracic,20–25 and cervical26–35 regions to assess pain that is suspected to be of discogenic origin. Discogenic pain is mechanical in nature (exacerbated with activity and relieved by rest) and is felt primarily in an axial distribution. Performing discography involves the injection of radiographic contrast into the nucleus of the intervertebral disc to visualize disc morphology (Fig. 17-1).4
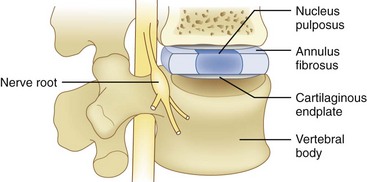
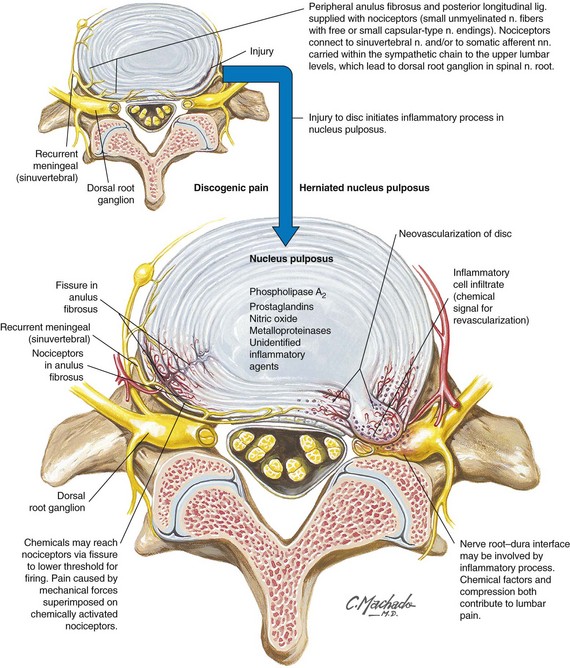
The prevalence of discogenic low back pain is 39% in those with low back pain persisting for at least 6 months and who have an unremarkable diagnostic workup and 26% of patients without radicular pain after facet joint pain was eliminated by either performing a diagnostic median branch nerve block or an intraarticular facet joint injection.36 The advent of new technology such as MRI, CT, and CT myelography has improved anatomical visualization of spine structures. However, these diagnostic modalities have not reliably identified the anatomical location of symptomatic spinal structures. This is evident in the individual who does not have radicular symptoms. Discs that appear normal or abnormal on MRI can either reproduce clinical symptoms during discography or be painless. The lumbar discs are innervated by branches from the lumbar ventral rami, the grey rami communicans, and the sinuvertebral nerve (Figs. 17-2 and 17-3). Lumbar discography has been postulated as a diagnostic test to elucidate the specific disc that requires disc excision and fusion with subsequent pain relief. The North American Spine Society (NASS) released its Position Statement on Discography in 198837 and again in 1995, summarizing the indications for discography. Both the International Spine Injection Society and NASS agree on the criteria for functional discography. Each organization indicates that a “chemically” sensitive disc is one that a patient feels pain at a low pressure stimulus (basically <15 psi). Between 15 and 50 psi, if a patient experiences pain that is concordant with the pathology of the painful disc, then it is deemed a pressure-sensitive disc. Pressures greater than 51 psi to 90 psi above the opening pressure are noted to be determined. A pressure above 90 psi is stated as being normal. The most common indication for lumbar discography is the need to determine whether one or more lumbar discs are responsible (i.e., the pain generator) for chronic ongoing low back pain. The study by Walsh et al38 refuted the findings by Holt19 demonstrating a 0% false-positive rate. Recent literature has demonstrated that compared with present imaging modalities, lumbar discography and lumbar CT discography are superior to MRI in determining abnormal annular pathology.39–43
Several studies have demonstrated the limitations of MRI compared with lumbar discography in identifying symptomatic versus asymptomatic discs.39–42 In 2000, Carragee et al44 challenged the concept of zero false-positive discography results on the grounds that abnormal psychometrics lead to misleading abnormal results. Manchikanti et al,45 in 2001, to the contrary, did not find any impact on discography results in those with or without a somatization disorder. Crock46 was the first to use the term internal disc disruption in 1970 to describe the clinical syndrome of axial low back pain secondary to pathological changes within the disc in the absence of a disc herniation. Radial fissures into the outer innervated annulus can cause pain because of mechanical or chemical irritation. This is the salient pathologic feature of internal disc disruption that cannot be detected on plain radiography, CT, or myelography because these studies are unable to detect internal disc abnormalities.
CT combined with discography allows the detection of annular pathology and determines if it is symptomatic or not. MRI can reveal annular pathology but cannot determine whether or not the disc is the pain generator (Fig. 17-2).38–41 Although the presence of a high intensity zone (HIZ) on T2-weighted MRI sagittal images in the posterior annulus (representative of a radial annular fissure) has a near 90% positive predictive value with concordant discography,34–36,38,39 this is not absolute, and the absence of an HIZ does not exclude annular pathology or discogenic low back pain.38–42 HIZ lesions are also found in patients without low back pain symptoms.47–49 Lumbar discography is not only important in identifying discs that are pain generators but also serves a key role in detecting whether abnormal or normal discs (based on imaging studies) are painful.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


