Chapter 54 Dreaming as a Mood-Regulation System
Abstract
That we feel and function better after a night of a sufficient number of hours of sleep has recently been supported in the Institute of Medicine report1 pointing out the negative impact on health and behavior of reducing the hours of sleep. A major focus of sleep research is investigating what it is about having 7 to 9 hours of sleep that restores physiologic and psychological functions. This is puzzling in light of the amount and regularity of rapid eye movement (REM) sleep—a complex state of high brain activation, motor inhibition, shutdown of afferent input, and experience of hallucinations2—and that it is REM sleep that is disproportionately reduced when total sleep hours are curtailed. This suggests that the loss of sufficient REM sleep, and the accompanying dreams, may well be implicated in some negative effects on health and behavior subsequent to widespread reduction in sleep hours.
The prevailing theory of dreaming at the time of the discovery of REM sleep was that of Freud3 who stated that dreams were a mechanism for the expression of primitive unacceptable drives, and that this display in sleep allowed these drives to be partially gratified, preventing their intrusion into waking life. There were few research tests of the validity of this theory. Foulkes4 undertook such a test by tracing the development of dreaming in normal children studied in the laboratory. He describes his findings on preschool aged children through to late adolescence, showing dreaming to be a cognitive skill parallel to the waking level of cognitive development, and concluded that this failed to support a unique drive-regulatory function of dreaming. Given that his method required a verbal report of the experienced dream, a difficult task even for some adults, Foulkes left open the possibility that REM sleep may perform this affect-modulating function before youngsters have the cognitive skill to communicate this experience.
Snyder5 extended the age group covered by Foulkes’s study by analyzing the content of the dreams of healthy young adults. His study provided two findings that contributed to the hypothesized mood-regulation function of dreams. The first was the presence in dreams of the dreamer as the main character in 95% of the reports from REM awakenings.5 The second was the direct expression of “unpleasant” emotion more than twice as often as pleasant emotion; fear and anxiety was the most common category, and anger was the next most common category.5
A common thread in current views of dream function is that dreams reflect recent emotion-related experience and connect this to the organized system of memories that define the self-concept. The recurrence of content patterns within the dreams of a night and between nights over time suggests that activation of dream images is not random. Globus proposed that “the periodic disturbances of REM … moves the [memory] networks towards … self consistency.”6, p. 134 Kramer7 tested this assertion using the Clyde Mood Scales8 before and after sleep and found that mood changed through the night and that dreaming seemed to be a problem-solving method that, when successful, resulted in increased happiness scores.7 Foulkes9 stated that “activation spreads according to preexisting patterns in symbolic memory” and “significant emotional life experiences may appear later in dreams when they serve as mnemonic references to those meaningful experiences organized by emotion.”9, p. 151 Thus there is some consensus that dreaming supports an identity-preserving function by downregulating affect that is disturbing to the organized self-system.
Mood-Regulation Function of Dreaming in Normal Persons
Evidence of Mood Regulation from Self-Reported Home Dreams
Some dreams are sufficiently unpleasant to abort sleep and awaken the sleeper prematurely with vivid recall of frightening content. This is the usual definition of a nightmare. Nightmares are common, affecting 2% to 6% of the overall population; are more frequent in children, women, and psychiatric patients; and have a negative relation to measures of mental health.10,11 Nightmare frequency compared between patients with and without laboratory-diagnosed insomnia found nightmares were more frequent in the insomnia group, but frequency was lower in those with reduced REM sleep.11 On a continuum of more unpleasant to more pleasant content, nightmares are at one extreme, bad dreams that do not wake the sleeper are at a mid point, and neutral or more pleasant dreams are at the opposite end. The frequency of the two types of unpleasant dreams correlate negatively with a self-report measure of well-being.12
Dreams recalled spontaneously by adults often have a negative affective tone. This contributes to their ability to be recalled. Individual differences in recall rates have been noted to be related to various personality traits and to specific states, although few of these correlations have stood up to replication. Dream recall has been noted to be higher in women and associated with a trait of their higher interest in their inner life. Recall has also been associated with a state of anxiety, which is linked to light sleep, higher rates of NREM dreams,13 and REM dreams with more intense negative affect. When these disturbing dreams exceed the capacity of sleep to contain them, a premature awakening from REM results in a failure of within-night mood regulation. However, failure to regulate negative mood on one night does not necessarily invalidate the mood-regulatory function. It might take more than one night to regulate a highly disturbing mood. Other possibilities are that the recall of negative dreams is an artifact of the method used to collect them. Researchers generally use questionnaires that ask for retrospective reports. A comparison of home dream reports to laboratory-collected dream reports show that home dream reports have more disturbing content.14
Because most sleep does not result in a premature REM awakening in fear, it is possible that dreaming is for the most part successful in regulating affect within the night or that the presleep affect might not require nightly regulating in healthy sleepers. In either case, waking without a change in mood when the mood was not elevated before sleep onset, or waking in a more positive mood when the presleep mood was only moderately elevated, was predicted in an early model of the relations of presleep mood, dream characteristics, and postsleep affect level.15 This model proposes:
A review of studies when presleep affect level is expected to be elevated in intensity and negative in type have been examined for their findings relevant to these proposals. Following the 1989 San Francisco earthquake, frequency of nightmares was reported to increase to 40% among persons who were living in the area but not in a control group living remotely in Arizona, where the rate was 5%.16 A traumatic event plus helplessness to cope with it were the conditions implicated in the persistence of nightmares over 4 or more years in children who had been kidnapped and buried in an abandoned quarry for 2 days.17 The author suggests that the long delay in dream adaptation was a function of the children’s having had no previous solutions to such an event stored in their long-term memory, which were necessary to provide helpful dream images to defuse their fear. Children who witnessed the 9/11 New York City Twin Towers attack, some from their preschool across the street, were studied by interviewing the parents, the teachers, and the children over 4 years. Those who continued to have disturbed dreaming had a higher rate of a previous personal trauma—tonsillectomy, car accident, or dog bite—than did exposed children who did not have nightmares. The authors suggested that those with previous traumas had been “sensitized” to attend to frightening events.18 Among adults surveyed by Internet for nightmare frequency following 9/11, only men reported a significant increase.10
Dreams Collected in the Sleep Laboratory
Dreams in Subjects Undergoing Surgery
Dream content reports were collected in the laboratory by Breger and colleagues19 before and after a planned stressful event: elective surgery. Although the dreams demonstrated the impact of surgery on the dreamers’ sense of personal integrity, this varied according to the meaning of this event to the person: whether it was anticipated to correct a problem or was a dreaded experience. This meaning was not directly represented in the dreams but was displayed metaphorically. This is one of the complications of dream research; the images are not realistic snapshots of waking events. They are more often compounds of new and old associated images and so require some unwrapping of their personal meaning. This poses problems for the reliability of scoring dream content. Winget and Kramer20 have provided a resource for this work in a book devoted to instruments for measuring dream content along with the reliability data available for each scale.
Dreams in Depressed Subjects
Sleep disorder clinicians have rarely applied sleep monitoring methods to study the dreams of patients presenting with various sleep disorders. Notable exceptions are work with major depression and nightmare patients. The finding that the classic timing of REM sleep is shifted to occur earlier in the sleep of those suffering a major mood disorder was noted by early sleep investigators.21,22 This was modeled as a phase advance of REM sleep by Wehr and coworkers23 and as a response to increased waking affect.24 There are other abnormalities of sleep in the depressed including an increased fragmentation of sleep, particularly of the REM periods. The percentage of rapid eye movements themselves is a good indicator of the general emotional or motivational turmoil in schizophrenics and in depressed patients.25 The density of rapid eye movements in REM episodes is more variable in the depressed subjects than in controls. These patients show periods when the eye movements are very sparse and periods of eye movement storms.
These abnormalities suggest an explanation for the why depressed subjects have difficulty developing or reporting coherent dreams and consequently fail to regulate morning mood. Dream recall in depressed subjects is poor, even when they are awakened from REM. Most common are reports of no recall or a short report describing a single image with flat affect.26–28 This poverty of dreaming may be due to the observed disturbances—the frequent interruptions of REM sleep and the dysregulation of the release of rapid eye movements, allowing too few to supply the images or too many to allow time for the associations necessary to construct a dream scenario. Nofzinger and colleagues29 reported that patients in remission from depression show a reduction in eye movement density. Other aspects of sleep in depressed subjects prove to be more stable. Two of these, the poor quality of sleep and early onset of REM, typically remain after remission.30,31 The most robust of the markers, the reduced latency to the first REM, appears to represent a genetic vulnerability to depression in family members.32
Indrusky and Rotenberg33 studied patients who had major depression and found mood change based on the patients’ self-report of their morning mood as worse, the same, or better than before sleep. When morning mood was “better,” the eye movement density was low in the first REM period and increased across the night to be highest in the last REM period. This is similar to the eye movement distribution pattern of healthy subjects. In contrast, those whose mood either did not change or worsened overnight had high eye movement density in the first REM and a slow decrease from REM to REM, the opposite to that of control sleepers. Thus depressed patients whose within-night sequence of rapid eye movement density resembles that of healthy subjects are more likely to feel an improvement of mood on awakening next morning. This is consistent with the findings of mood improvement with this pattern reported by others.30,34
Dreams in Divorcing Subjects
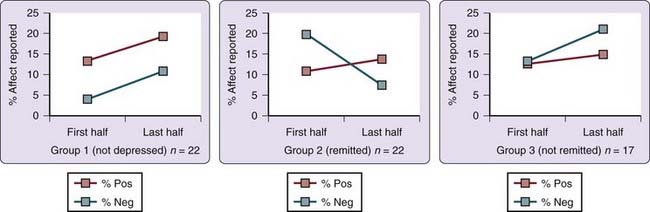
Clinical depression is common and has a strong effect on both sleep and dreaming. In one study of this series24,30,35–37 equal numbers of male and female subjects, 40 with untreated clinical depression secondary to the divorce and 30 nondepressed controls, were studied in the laboratory, with REM dreams collected at intake and, for 22 of 30 controls and 39 of 40 depressed subjects, 1 year later. Subjects rated their dream affect as pleasant, unpleasant, or neutral and whether the dream was unemotional, mildly emotional, or strongly emotional. The number of unpleasant dreams was significantly higher in the depressed group. Depressed subjects who dreamed of the ex-spouse were not more depressed than those who did not but had higher dream affect scores and no longer met depression criteria at the 1-year reassessment. Those who dreamed of the former partner with expressed emotion on the first REM collection night showed a within-the-night dream affect change from negative to positive. The difference in percentage of positive and negative affect ratings in the dream reports of the first half night and those in the second are seen in Figure 54-1. The discriminant function analysis testing whether the order of dream affect predicted remission from depression was highly significant. This within-sleep change in dream affect correctly classified the remission status of 72% of those initially depressed.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


