Enlarged Deep (Medullary/Ependymal) Veins
James D. Eastwood, MD
DIFFERENTIAL DIAGNOSIS
Common
Developmental Venous Anomaly
Arteriovenous Malformation
Less Common
Sturge-Weber Syndrome
Thrombosis, Deep Cerebral Venous
Thrombosis, Dural Sinus
Dural A-V Fistula
Glioblastoma Multiforme
Intracranial Hypotension
Rare but Important
Capillary Telangiectasia
Blue Rubber Bleb Nevus Syndrome
Dural Venous Sinus Stenosis
Vein of Galen Malformation
Demyelinating Disease, NOS
Lymphoma, Intravascular (Angiocentric)
Encephalitis (Miscellaneous)
Granulomatous Angiitis
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Urgent: Look for deep (i.e., internal cerebral) vein or dural sinus occlusion!
If not venous occlusion, consider
Could the lesion be a DVA?
Are there prominent cortical vessels as well?
Is there associated cortical abnormality?
Helpful Clues for Common Diagnoses
Developmental Venous Anomaly
Enlarged medullary veins
Drains into single dominant transcortical vein
Empties into dural sinus or deep ependymal vein
Solitary unless blue rubber bleb nevus syndrome
Hemorrhage rare unless associated with cavernous malformation
Arteriovenous Malformation
Parenchymal nidus, prominent cortical vessels
Enlarged medullary veins less common
Deep (subependymal) drainage associated with ↑ hemorrhage risk
On T1 C+ small AVMs may appear as focal “blush” & draining vein
Helpful Clues for Less Common Diagnoses
Sturge-Weber Syndrome
Facial hemangioma ipsilateral to leptomeningeal (pial) angiomatosis
Paucity of normal cortical venous drainage causes chronic venous ischemia
NECT: Cortical Ca++, atrophy
CECT/T1 C+ MR
Enhancing pial angioma
Enlarged medullary veins
Enlarged choroid plexus ipsilateral to malformation common
FLAIR MR: “Ivy sign” of ↑ sulcal signal
Thrombosis, Deep Cerebral Venous
Usually affects both internal cerebral veins (ICVs) ± vein of Galen (VOG), straight sinus (SS)
Initial findings may be subtle!
NECT
Hyperdense ICVs ± VOG, SS
Hypodense thalami, basal ganglia, ± deep white matter
± Petechial hemorrhages
CECT
“Empty delta sign” if clotted SS, venous confluence
May see irregular “shaggy” enhancement around ventricles from engorged medullary veins
MR
T1: Deep veins iso- to hyperintense
T2: Hypointense clot may mimic “flow voids”
T2/FLAIR: Bilateral basal ganglia, thalami hyperintensities
T2* (GRE/SWI): Best sequence; clots “bloom”
T1 C+: Deep medullary veins may enlarge, enhance
DSA
Absent ICVs ± nonfilling of VOG, SS
Thrombosis, Dural Sinus
Chronic superior sagittal sinus occlusion → medullary, ependymal veins enlarge as collateral venous drainage
Can mimic blue rubber bleb nevus syndrome
Dural A-V Fistula
Higher Cognard grades (IIB and above)
Enlarged cortical > > medullary veins
Increased flow voids near or in dural venous sinus
Glioblastoma Multiforme
GBM, other malignant gliomas may develop necrosis, prominent neovascularity
Draining deep white matter (medullary, ependymal) veins may become very prominent
Intracranial Hypotension
Orthostatic headaches
Look for “sagging” floor of 3rd on sagittal, tonsillar herniation
Passive dural venous congestion common; medullary/deep ependymal vein enlargement less common
Helpful Clues for Rare Diagnoses
Capillary Telangiectasia
Large capillary telangiectasia (typically > 1 cm) may have prominent central draining vein
Best seen on T1 C+ scan
Becomes hypointense on T2* (GRE/SWI) images
Blue Rubber Bleb Nevus Syndrome
Multiple cutaneous (bluish venous “blebs”), GI hemangiomas
Diverse CNS vascular malformations, venous variants common
Multiple DVAs classic
Variant: Sinus pericranii & multiple DVAs
Dural Venous Sinus Stenosis
Patients often have undiagnosed source of severe chronic recurrent headaches
Increased collateral flow, venous prominence, variable ↑ ICP
Vein of Galen Malformation
Infant/child with dilated VOG
Enlarged ICVs, ependymal veins > > medullary veins
Demyelinating Disease, NOS
Fulminant demyelinating disease
Causes acute perivenular inflammation
Increased blood flow, loss of normal BBB
MS, ADEM, acute necrotizing/hemorrhagic leukoencephalopathy variants
Enhancement of deep medullary veins may be very prominent
Lymphoma, Intravascular (Angiocentric)
Clinical presentation
Stroke-like symptoms
Less common: Dementia, progressive mental status decline
Intravascular tumor plugs ± extension into perivascular spaces
Punctate, linear enhancing foci
Encephalitis (Miscellaneous)
Parenchymal T2/FLAIR abnormality ± mild-moderate enhancement
Granulomatous Angiitis
Enhancing foci ± mass effect
May have striking deep perivenular enhancement
Image Gallery
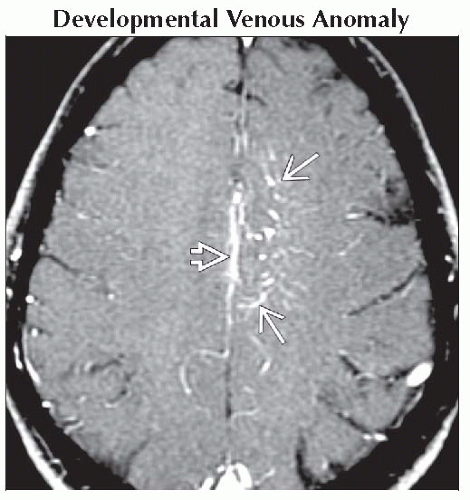 Axial T1 C+ MR shows prominent medullary tributaries
 of deep DVA. Prominent septal, internal cerebral, subependymal roof veins of deep DVA. Prominent septal, internal cerebral, subependymal roof veins  drained lesion. This was an incidental finding. drained lesion. This was an incidental finding.Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|