CHAPTER 136 Epidermoid, Dermoid, and Neurenteric Cysts
Recent developments in understanding the embryogenesis of complex dysraphic malformations suggest that the three central nervous system (CNS) entities epidermoid, dermoid, and neurenteric cysts all reflect a problem at the gastrulation stage of development and consist of primary disruption of tissues derived from one or more of the three germ cell layers.1–3 Thus, dermoid and epidermoid cysts, as well as dermal sinus tracts, reflect an abnormality of surface ectoderm, and neurenteric cysts are a type of endodermal malformation. All three disorders are frequently associated with one or more of the mesodermal malformations, particularly those involving the vertebrae (e.g., hemivertebrae, absent vertebrae, fused vertebrae, butterfly vertebrae, midline bony spurs).
Epidermoid Cysts
Epidermoid cysts or tumors are benign lesions that may arise in the spine or intracranially. They may be intradural (usually extra-axial) or extradural (usually arising in the diploic space of the calvaria). Intracranial epidermoid cysts account for 0.2% to 1.8% of all intracranial tumors.4,5 They generally occur in the cerebellopontine angle or in the parasellar cisterns.6–8 Most intraspinal epidermoid cysts are subdural and extramedullary, but they can rarely develop in the intramedullary compartment.9,10 In 1936, Love and Kernohan first described epidermoid and dermoid cysts as congenital epithelial tumors.11 However, it has been widely held that these tumors derive from ectopic inclusions of epithelial cells during neural tube closure.12 More recently, Dias and Walker explained their cause as primarily being a gastrulation dysembryogenesis,3 with secondary disruption of neural tube closure during the third to fifth week of gestation.13 Epidermoid and dermoid cysts represent malformations of surface ectoderm (as opposed to neuroectoderm) in this schema.
Clinical Findings
Epidermoid tumors have been reported in patients from infancy to adulthood and have been incidental findings at autopsy.11 They may be cranial or spinal in location. The average age at detection is 40 years.4 The tumors usually grow linearly, similar to normal skin, and thus have an insidious onset.14 The symptoms and signs are variable and depend on tumor location. Extradural lesions are often manifested as a local mass, with or without headache.12 Intradural tumors are more likely to be associated with headache (because of the common parasellar location), visual disturbance, and to a lesser extent, hypothalamic alterations. Tumors in the middle fossa grow quite insidiously and are often asymptomatic, whereas those in the cerebellopontine angle may cause ataxia, dizziness, or local cranial nerve deficits.4 Twenty years of trigeminal numbness was the initial complaint in a patient with a large middle fossa–petrous apex–Meckel’s cave interdural (between the dural leaves) epidermoid.15 A picture of acute meningitis may indicate epidermoid cyst rupture. Spinal epidermoid tumors are frequently associated with vertebral anomalies.3,11
In their classic 1936 paper on epidermoid and dermoid tumors, Love and Kernohan described 15 patients, 10 of whom had epidermoid tumors.11 Seven of these tumors were intradural, and 3 were extradural. Almost 60 years later, Gormley and colleagues reported their experience with 32 tumors, 22 of which were epidermoids (16 intradural and 6 extradural).12 The initial symptoms and signs in both series were amazingly similar. The duration of symptoms is long for epidermoid tumors, an average of 16 years in the series of Love and Kernohan.11 Recently, Akar and coauthors reported their experience with 28 cases of intracranial epidermoid tumor, 17 of which were in the cerebellopontine angle, 2 in the fourth ventricle, 1 in the cisterna magna, 4 in the sylvian fissure, 2 in the occipital lobe, 1 in the lateral ventricle, and 1 in the intradiploic space.4 The median duration of symptoms was 4.6 years.
Imaging
With the advent of CT, intradural epidermoid tumors could be more accurately diagnosed. Typical CT findings consist of a homogeneous nonenhancing hypodense lesion in the subarachnoid space without surrounding edema. The differential diagnosis includes arachnoid cyst, Rathke’s cleft cyst, craniopharyngioma, and other cystic tumors, with arachnoid cysts being the most problematic. Careful evaluation of Hounsfield units may show the lesion to have more fat density than cerebrospinal fluid (CSF) density. Epidermoid tumors more often extend into the subarachnoid space and enlarge it, unlike arachnoid cysts, which cause a more focal mass effect. Occasionally, epidermoids are seen as high-density masses (“white epidermoids”) on CT images, which can make diagnosis difficult.2,5
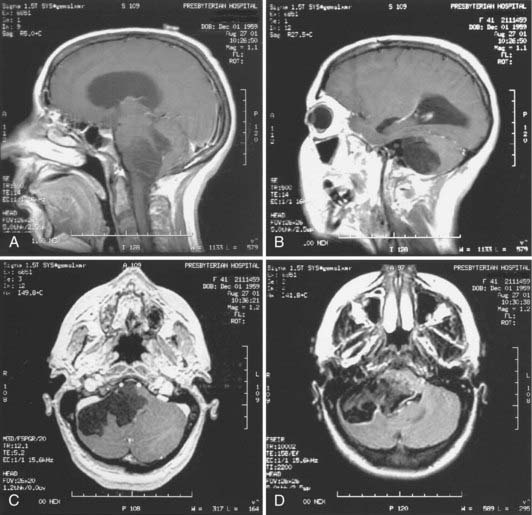
Magnetic resonance imaging (MRI) is now the tool of choice for diagnosing these lesions. Signal intensity patterns are variable, ranging from hypointense to hyperintense, and the tumors are frequently multiloculated. Typically, the tumor signal is heterogeneous and most often shows hypointensity on T1-weighted images and hyperintensity on T2-weighted images.2,7 There may be a rim of high signal intensity visible on proton density studies; some tumors show rim enhancement with gadolinium administration (Fig. 136-1). The differential diagnosis again includes the cystic entities described earlier. It is difficult to distinguish epidermoids from arachnoid cysts on standard and spin echo MRI pulse sequences, but diffusion-weighted (DW), fluid-attenuated inversion recovery (FLAIR), constructive interference in the steady state, and fast imaging with steady-state precession studies can often differentiate between epidermoid tumors and the CSF within arachnoid cysts.16 There is usually no edema of the surrounding parenchyma, and hydrocephalus is rare, even in the setting of large tumors and brain displacement. In a radiographic series of 23 intracranial epidermoids, Kallmes and coauthors reported 14 tumors in the cerebellopontine angle, 6 (43%) of which extended into Meckel’s cave.17 Hakyemez and colleagues conducted a prospective radiologic study comparing DW with spin echo and FLAIR sequences in the evaluation of 15 patients with intracranial epidermoid cysts.16 They found that FLAIR sequencing was superior to the use of conventional MRI in demonstrating the epidermoid cysts and that DW imaging was superior to other types of MRI sequencing in delineating the borders of the epidermoid cysts.
Treatment
Symptomatic patients benefit from surgery, but it is often technically difficult because of tumor adhesions insinuating themselves among adjacent structures. The tumor is well demarcated, with a smooth, hypovascular capsule. The cyst contains characteristic pearly flakes. Current recommendations for the surgical approach are similar to those promulgated by Love and Kernohan in 1936,11 including primary intracapsular debulking and subsequent removal of the capsule. The surgical ultrasonic aspirator is extremely useful in the operative management of these tumors. Fragments of capsule adherent to important structures are left when necessary to avoid neural or vascular injury. Although subtotal resection increases the risk for recurrence, the slow growth of epidermoid cysts makes this less problematic. The capsule should not be removed from intramedullary cysts because of the risk of causing neurological deficits.10
Much has been written and said about the risk for chemical meningitis associated with intraoperative spillage of cyst contents or preoperative cyst rupture. This has also been reported as a radiographic finding of small fat globules in the subarachnoid and intraventricular spaces.4 Steroid administration is useful in the treatment of meningitis, but hydrocephalus may ensue and require shunting. At this time, there is no established role for radiotherapy or chemotherapy in the treatment of residual or recurrent epidermoid cysts.
Pathology
Epidermoid cysts are benign and consist of a thin capsule of stratified, keratinized squamous epithelium. The cyst contains an accumulation of desquamated epithelial cells, keratin, and cholesterol. Malignant transformation in these tumors is rare, but squamous cell carcinoma has been reported to arise from an epidermoid cyst.18 Fifteen cases of leptomeningeal dissemination of squamous cell carcinoma arising in an epidermoid cyst have been reported, only four of which demonstrated malignant cells within the CSF.19 A malignant melanoma has also been reported in a temporal lobe epidermoid.14 Immunohistochemical staining for the carbohydrate antigen CA19-9 has been positive in intracranial epidermoids.20 Positive staining for CA19-9 occurred in epithelial cells in the cyst wall in two of four patients with intracranial epidermoids, as well as in the subepithelial collagenous tissue and keratinous tissue.20 This tumor marker, originally developed as a colon cancer antigen, is also detected in the serum of patients with epidermoid tumors. Takeshita and coworkers reported one patient who underwent incomplete tumor resection and whose postoperative CA19-9 serum levels remained elevated but lower than preoperative levels.20 Thus, serum antigen levels can be used to evaluate patients for tumor recurrence or progression.
Dermoid Cysts
Dermoid cysts share many characteristics with epidermoid cysts. They are also clinically and biologically benign, with the main problem at initial evaluation being related to mass effect on neural structures in a tight space (intracranial or spinal). They represent a developmental malformation, with the defect in gastrulation affecting the surface ectoderm and causing a secondary disruption of neural tube closure.3 An interesting case report of monozygotic twins—one with a cerebellar dermoid tumor and an occipital dermal sinus tract and the other with an occipital meningocele and cerebellar aplasia—supports the theory that the malformation occurs at the gastrulation phase with secondary dysraphism.21 Epidermoid cysts contain epithelial cell debris and keratin, whereas dermoids contain elements of the dermis, such as hair and hair follicles and apocrine, sebaceous, or sweat glands. Intracranial dermoids are rare congenital lesions that account for 0.04% to 0.6% of all intracranial tumors. They tend to occur at the midline and, when extradural, may arise at the anterior fontanelle.1,21
Clinical Findings
Patients with dermoid cysts are generally seen at a younger age than those with epidermoids. Gormley and coworkers noted an average age at diagnosis of 15 years for dermoid cysts versus 35 years for epidermoids.12 In the study by Love and Kernohan, the duration of symptoms averaged 8.5 years in patients with dermoid tumors and 16 years in those with epidermoid tumors.11 Their 15-patient series consisted of five dermoid tumors: three intracranial-intradural, one spinal-intramedullary, and one calvarial-extradural. Dermoid cysts are usually found at the midline. As with epidermoid cysts, there is a female preponderance, and patients may initially be seen with local neural deficits, headache, or meningitis.12 Dermoid tumors have been reported in association with Klippel-Feil syndrome.22






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


