Chapter 10 Gait disorders
Pathophysiology and clinical syndromes
Balance
It is important to distinguish between balance and stance. Stance is the posture of standing. It is normally upright on two legs with a distance between the feet approximately equal to pelvic width. An example of abnormal stance would be the stooped posture seen in Parkinson disease. Balance is the ability to maintain stance without falling or excessive lurching (Benvenuti, 2001). If balance is poor, sometimes persons modify their stance; the most common manifestation is increasing the distance between the feet to widen the base of support (BOS).
From standard Newtonian physics, for an object to maintain its position, its center of mass (COM) must be over its BOS. In the case of a human standing, the COM is generally somewhere in the abdomen and the BOS is the area between and including the feet. Since the BOS is relatively small and the COM relatively high above the BOS, it takes considerable skill to maintain the BOS above the COM. Recently, it was recognized that the ability to remain upright cannot be explained best by just the simple need to maintain the BOS above the COM. This is a static requirement, and the body or body parts are constantly moving. This movement must be taken into account. A “dynamic model” of balance includes consideration of the velocity of COM (Pai et al., 1998). The general principle is that the balance mechanisms of the body (such as the postural muscles) must be able to counteract any large velocities of the COM, even if the COM is currently over the BOS, since if they cannot, the COM will soon be beyond the BOS.
The body is constantly moving and this movement is called sway. Each body part can have its own movement, but the important “summary” of these movements would be movement of the COM for the reasons already described. Neurologists are used to doing a visual analysis of sway, but this is not very exact, of course. Instrumental methods have been developed. The position of the COM can be estimated although it is generally somewhat difficult. The position of the different body parts can be determined with video methods, and if their individual masses are estimated, then the COM can be calculated. This is generally done only in research laboratories. An alternative method, generally called posturography, comes from the ability to record forces that the body exerts on the floor with devices called force plates (Kaufman et al., 2001). The devices measure force in three directions, vertical, forward/backward, and side-to-side, and the two-dimensional center of action of the forward/backward and side-to-side force is called the center of pressure (COP). In the static situation, the COM is directly over the COP. Movements of the COM cause deviance of the matching of the COM and COP, but if the movements are small and slow, the deviance is not much. For this reason, sway is often measured with movements of the COP.
Generally it is thought that more sway means less good balance. This is often but not always true. In some circumstances, because the balance is bad, patients stiffen up, voluntarily or involuntarily, and the sway might decrease. This might be true in Parkinson disease, for example (Panzer et al., 1990). When a patient is “off,” balance is poor and patients are very stiff, often swaying little. When the patient is “on,” balance is better, the patient is more relaxed and sway might increase. Sway markedly increases with dyskinesias (characteristic of the “on” state and good balance). In most circumstances, however, increased sway does indeed indicate poor balance and posturography can be employed to make this assessment quantitatively. A surer way to assess balance is to see what happens with a perturbation to stance. If patients can remain upright, then balance is good; if they fall, balance is defective. This is the logic of the pull test.
The pull test is done by having the patient stand and having the investigator stand behind the patient and give a sudden pull backward. The patient is told to maintain balance. The best ability is to deal with the perturbation by body movements without moving the feet. A second-level ability is to maintain balance by taking a timely step backward. Failure, of course, is a fall, and that is the reason that the test is a pull rather than a push; the patient can fall into the examiner. Balance is virtually always better in the forward direction than the backward direction. With poor balance, patients tend to fall backward. All the reasons for this are not clear, but one is likely that when standing, the COM is closer to the back of the foot than the front. In any event, because of this, the pull test is often only done in the backward direction. A related test called the push and release test has been suggested, and it might be more sensitive and consistent than the pull test, but it has not been much utilized (Jacobs et al., 2006).
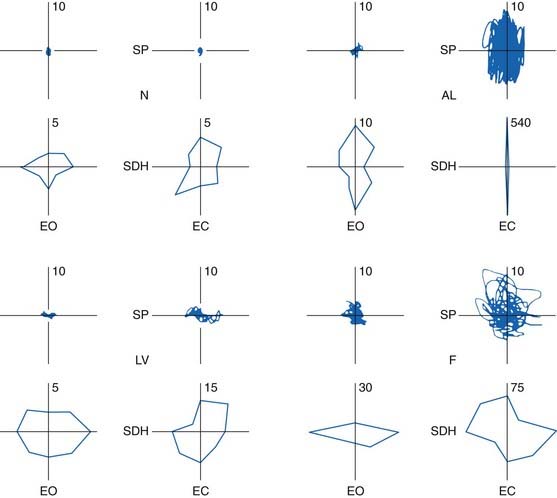
Abnormalities in posturography have been reported in many disorders. The best studied has been cerebellar disturbances (Diener et al., 1984; Gatev et al., 1996); the findings are reviewed in detail in Chapter 2 and illustrated as an example here (Fig. 10.1).
Gait
Human gait is a complex, rhythmic, cyclic movement (Winter, 1991). The movements are generated to some extent by a locomotor generator in the spinal cord, but they are under control by supraspinal mechanisms. The spinal cord generator can produce only simple, primitive stepping and react to perturbations in stereotypic fashion (Burke, 2001). Supraspinal mechanisms are required for a person to go in desired directions, with desired velocities and to deal well with perturbations. An important supraspinal control center is the mesencephalic locomotor region, which includes the pedunculopontine nucleus (PPN). The PPN is an important integrator of activity from basal ganglia, cerebellum, and motor cortex and projects to reticular nuclei in the brainstem. The fastigial nucleus of the cerebellum seems also important (Mori et al., 2001). Supraspinal control signals are conveyed to the spinal cord by reticulospinal and vestibulospinal tracts.
There are a number of terms that are useful in describing gait, and many of them are defined below.
A gait cycle for the right leg is illustrated in Figure 10.2. Note that the gait cycle for the left leg is not exactly 180° out of phase. For this reason, and because stance phase is longer than swing phase, there are several periods where both feet are on the ground, and these are called double support. (In normal walking, there are no periods of simultaneous swing; that is, no “flying,” but this may occur with running.) With normal gait, when the foot contacts the ground, the heel contacts first and then the foot rotates to flat with the heel as the point of rotation. When the foot leaves the floor for swing, the foot rotates over the toe and the heel leaves the ground first.
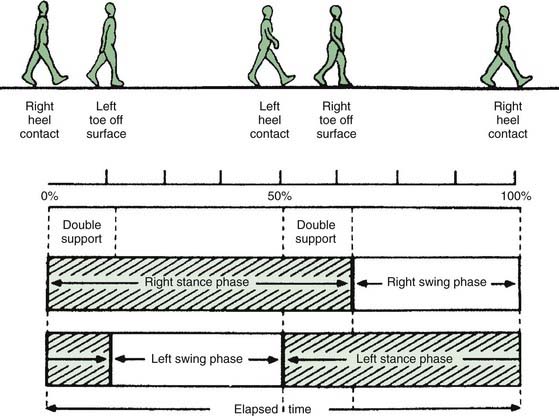
Figure 10.2 Diagram of the gait cycle; see text for detailed description.
From Sudarsky L. Geriatrics: gait disorders in the elderly. N Engl J Med 1990;322(20):1441–1446, with permission.
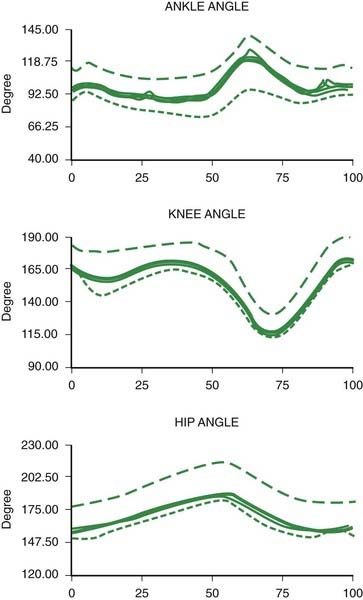
The joint angles of a normal gait cycle are illustrated in Figure 10.3. The ankle shows a brief plantar flexion at heel strike, followed by a gentle dorsiflexion in stance as the body moves over the foot. The ankle then shows a brisk plantar flexion producing push-off lasting from heel off to toe off. During swing there is a dorsiflexion of the ankle to avoid hitting the toe on the ground and to prepare for heel strike. The knee shows a slight flexion during stance and a more pronounced flexion during swing. The hip extends in stance and flexes during swing.
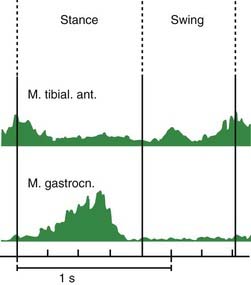
Muscle activities during gait are illustrated in Figure 10.4. During the gait cycle, the triceps surae (gastrocnemius-soleus) is active primarily at the end of stance to push off for the swing phase. The tibialis anterior muscle is active in the beginning of stance to slow the plantarflexion of the foot so that it does not slap onto the floor. Then it is active again during swing to produce the dorsiflexion of the ankle mentioned above.
Gait initiation
The initiation of gait is a special problem (Elble et al., 1994). Not only does it pose a unique biomechanical problem, it also causes some patients particular difficulty (Mancini et al., 2009). The task is to get the body moving forward and to get the first foot off the ground into a “swing phase.” In quiet standing, there is a very slight tonic activation of the triceps surae. This prevents the body from falling forward since the COM is anterior to the ankle joints. The first event is a diminution of activity in the triceps surae muscles, more prominent on the side of the leg that will become the stance leg for the first step. This by itself would cause the body to start moving forward, rotating around the ankle. Then, the tibialis anterior muscles contract, which actively rotates the body forward around the ankle. These events get the body moving.
Gait disorders
Epidemiology
Gait problems are a major neurologic problem, particularly in elderly people (Sudarsky, 2001). In this population, common causes for problems are stroke, peripheral neuropathy, brain or spinal cord trauma, and Parkinson disease. The term “senile gait” is sometimes used, but it likely does not exist as a distinct entity. Multiple medical problems accumulate with age, including visual difficulties and arthritis, that become additive.
Sudarsky (1997) evaluated a series of patients referred for an unknown gait disorder. After careful neurologic evaluation, he was able to make a diagnosis in most (Table 10.1). The most frequent entities were sensory deficits, myelopathy, multiple infarcts, parkinsonism, and unknown.
Table 10.1 Frequency of etiologies of neurologically referred undiagnosed gait disorders
| Sensory deficits | 18.3% |
| Myelopathy | 16.7% |
| Multiple infarcts | 15.0% |
| Unknown | 14.2% |
| Parkinsonism | 11.7% |
| Cerebellar degeneration | 6.7% |
| Hydrocephalus | 6.7% |
| Psychogenic | 3.3% |
| Other | 7.5% |
“Other” etiologies include metabolic encephalopathy, antidepressant and sedative drugs, toxic disorders, brain tumor, and subdural hematoma.
From Sudarsky L. Clinical approaches to gait disorders of aging. In: Masdeu J, Sudarsky L, Wolfson L, eds. Gait Disorders of Aging: Falls and Therapeutic Strategies. Philadelphia: Lippincott-Raven; 1997, pp. 147–158, with permission.
Evaluation of gait
There are a number of important observations that have implications for the differential diagnosis (Nutt et al., 1993):
Veering
Deviations from a direct line of progression are due to either vestibular or cerebellar disorders.
Freezing
Freezing is also known as motor blocks and is characterized by lack of movement with the feet looking like they are glued to the floor (Snijders et al., 2008; Browner and Giladi, 2010). Patients often look like they are trying to move, but they cannot. This may be due to inability to generate sufficient postural shifting to initiate forward movement (Elble et al., 1996; Mancini et al., 2009). Freezing can occur when trying to initiate gait, in which circumstance it has also been called “start hesitation.” Freezing can also interrupt walking, and in this circumstance is sometimes precipitated by a sensory stimulus such as a doorway, the ring of a doorbell, or a street light changing color. Curiously, sensory stimuli can also be used to improve freezing. They appear to act in this regard by providing external triggers for movement.
The pathophysiology of freezing is not clear, but there are a number of associated abnormalities. Patients show defective bilateral coordination of stepping (Plotnik et al., 2008). There is an association of freezing with loss of frontal lobe executive function (Amboni et al., 2008). Another possible factor is the sequence effect where sequential movements become progressively smaller (Iansek et al., 2006; Chee et al., 2009). One study showed that freezing would occur when the demands for rapid stepping were high (Moreau et al., 2008a). Yet another factor contributing to freezing is the excessive dependence on external stimuli in patients with PD (Hallett, 2008). Imaging studies suggest that freezing is associated with abnormalities of the mesencephalic locomotor region (Snijders et al., 2011).
In addition to the absence of movement, another form of freezing is characterized by rapid, side-to-side shifting of weight, but no lifting of the feet and no forward progression. This has been called the “slipping clutch syndrome.” In this situation, physiologic studies show co-contraction activity in antagonist muscles, apparently not permitting effective forward movement (Yanagisawa et al., 2001).
Freezing is very common in idiopathic PD, but is also seen in other parkinsonian states such as progressive supranuclear palsy, vascular parkinsonism, and normal pressure hydrocephalus. It seems less common in multiple system atrophy and drug-induced parkinsonism (Giladi, 2001).

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


