Chapter 2 History of Spinal Instrumentation
The Modern Era
Dorsal Thoracolumbar Instrumentation
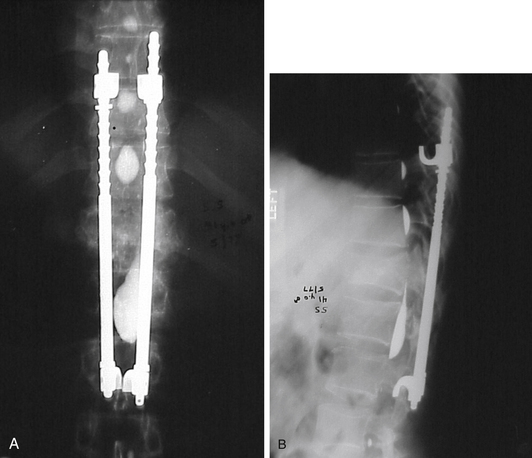
In 1975, the Harrington rod represented the state of the art in spinal instrumentation. The rod system, originally developed by Paul Harrington for the correction of spinal deformities, was soon used in the treatment of traumatic injuries1,2 (Fig. 2-1), degenerative disease,3 and metastatic disease.4,5 The system provided distraction rods as well as compression rods and hooks. Over the years, however, their widespread use led to recognition of their limitations. The use of a distraction system provided excellent correction of coronal plane deformities (scoliosis). Unfortunately, the use of distraction as the sole correction tool resulted in the loss of normal sagittal plane alignment. The loss of normal lumbar lordosis was associated with “flat back syndrome.”6,7 Hook dislodgement and rod breakage also proved to be troublesome complications.8,9 In addition, casting or bracing was generally required in the postoperative period, which proved to be difficult or impractical in some patients.10
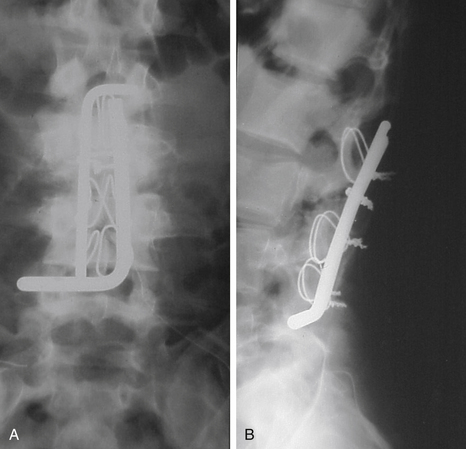
Luque popularized the use of a  -inch steel rod secured at each spinal level with sublaminar wires (Fig. 2-2). Luque reasoned that increasing the number of fixation points along a construct would reduce the force placed upon each individual point and obviate the need for a postoperative cast or brace. Additional beneficial effects of segmental fixation were that it increased the potential corrective power of instrumentation, reduced the potential for construct failure, and resulted in improved fusion rates.
-inch steel rod secured at each spinal level with sublaminar wires (Fig. 2-2). Luque reasoned that increasing the number of fixation points along a construct would reduce the force placed upon each individual point and obviate the need for a postoperative cast or brace. Additional beneficial effects of segmental fixation were that it increased the potential corrective power of instrumentation, reduced the potential for construct failure, and resulted in improved fusion rates.
Although the corrective power of sublaminar wires was well-appreciated, many surgeons had reservations in using them because of reports of neurologic injury resulting either from direct trauma or from epidural hematoma.11,12 In addition, revision surgery to alter sublaminar wiring is problematic because scarring may preclude the passage of new wires at the same laminae. In response to these concerns, Drummond et al.13 developed a method for segmental fixation using a button-wire implant passed through the base of the spinous process. This technique does not provide as strong fixation as do sublaminar wires. It avoids, however, passing anything into the spinal canal and thus reduces the risk of direct neurologic injury. This compromise of fixation for less risk of neurologic injury was seen as a prudent choice by many surgeons operating on healthy, neurologically normal adolescents with idiopathic scoliosis. Nevertheless, some pundits referred to the procedure as the “chicken-Luque” procedure.
Increasingly sophisticated multiple hook-rod systems appeared in the 1980s that provided much of the strength of wire fixation but with greater flexibility to address deformities in both the sagittal and the coronal dimensions. The Cotrel Dubousset (CD) system was introduced into the United States in 1986 using a ¼-inch rough-surfaced rod.14 Multiple hooks allowed spinal surgeons to apply compression and distraction over different areas within the same rod. The multiple-hook design applied the principles of segmental fixation without the need for sublaminar wires. Significantly, the system provided for a unique mechanism for deformity correction: rod rotation. This proved a powerful force in the correction of scoliosis. Further stability was provided by cross-linking the two parallel rods together.
The advantages of the CD system were partially offset, however, by the difficulty of removing it. The locking mechanism of the hooks was irreversible without destroying the hook or cutting the rod. The Texas Scottish Rite Hospital (TSRH) system was a design advance that addressed the issue of revision surgery. It was similar to the CD system in its use of multiple hooks and cross links but was designed to allow for the removal of the system’s individual components if necessary. Although the features of the TSRH system simplified revision surgery, the top-loading side-tightened system was not universally appreciated. After maturation of the fusion mass, the side-tightened bolts were not always accessible. The following decade saw the introduction of numerous, similar dual-rod systems like Moss-Miami and Isola.6,15 The major variations revolved around the leading and locking mechanisms: side loading, top loading, side tightening, or top tightening. The last decade has seen the introduction of numerous systems that operate with the same design principles, with a shift toward the use of polyaxial screws that make coupling of the fixation points to the rods easier. Today’s systems often have a wide range of screw choices, including monoaxial, polyaxial, uniaxial (screws that are mobile in only one plane to allow for better derotation), as well as monaxial, polyaxial, and uniaxial reduction screws (screws with extended tabs, which allow gradual reduction of the rod into the body of the screw).
A major advance provided by these spinal systems was the exploitation of the pedicle as a site for segmental fixation. This innovation is generally credited to Roy-Camille of Paris. Roy-Camille performed his first operation in 1963 but did not publish the results until 1970.16 Pedicle screws presented many advantages when compared with other tools for spinal fixation. Pedicle screws are biomechanically superior as a point of fixation17 compared with hook- or wire-rod constructs and can be placed into the sacrum, an area to which fixation is otherwise difficult. In addition, they can be placed even after a laminectomy has been performed and can be positioned without entering the spinal canal.18 This advantage allowed for the massive proliferation of spinal instrumentation into the area of degenerative spinal disorders. Prior to the advent of pedicle-screw instrumentation systems, there had been only sporadic reports of the use of instrumentation for degenerative spinal disorders. The Knodt rod (a small distraction rod system) had been used previously in degenerative disease but was associated with localized loss of lordosis and device dislodgement. In addition, the system needed some lamina for device fixation. Pedicle-screw systems, however, can be used after a total laminectomy.
Arthur Steffee popularized the use of pedicle screws in the United States in 1984 using a contourable plate. At about the same time, a screw-rod system, developed by Yves Cotrel of France, was in use in Europe that became incorporated into the “Universal” CD system. Controversy soon followed, with both the screw-plate and screw-rod constructs developing a group of proponents.19 Proponents of plates noted that plates were stronger. Most surgeons were ultimately attracted, however, to rods because their use provides greater flexibility, reduces encroachment upon the adjacent facet joints, and leaves more surface area for fusion. The marriage of the long dual-rod constructs to lumbar pedicle screws was an important development that enhanced the surgeon’s ability to accomplish increasingly difficult and complex spinal reconstructions. The use of the polyaxial pedicle screw has further advanced the ease of spinal reconstructions.
In recent years, there has been an interest in developing dynamic stabilization systems for degenerative diseases. The impetus for these systems arises from clinical evidence suggesting that 100% spinal fusion does not correlate with good clinical outcomes, which may range from 60% to 80%.20 Spinal fusion may also have kinematic and kinetic consequences at adjacent segments that may increase the rate of adjacent level degeneration.21 Dynamic stabilization systems aim to restore functional stability while maintaining intersegmental motion.
The most notable advancements in pedicle screw-rod based systems are the Graf ligmentoplasty system, the Isobar TTL Semi-rigid spinal system (Scient’X, West Chester, PA), and the Dynesys system (Zimmer Spine, Minneapolis, MN). The Isobar TTL and the Dynesys have Food and Drug Administration (FDA) approval as an adjunct to fusion, but to date none of these systems have been approved as a dynamic stabilizer (i.e., without fusion).20–24 The Dynesys system was the only device to undergo an FDA Investigational Device Exemptions (IDE) study as a dynamic stabilizer. The system is composed of titanium pedicle screws connected via a terephthalate cord and polycarbonate spacer. Several authors have recently reported mostly favorable results with a variable incidence of complications.25–31 At the time of this writing, no system has demonstrated enough evidence to justify widespread use or to be the gold standard.
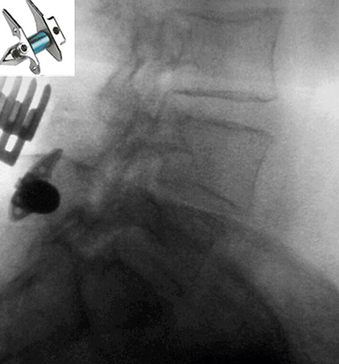
Interspinous devices that increase the intervertebral space have also been developed to treat a myriad of degenerative conditions. These devices can be categorized as static or dynamic.32 The most noteworthy static devices include the X STOP (Saint Francis Medical Technologies Inc., Alameda, CA), ExtenSure (NuVasive Inc., San Diego, CA), and Wallis implants (Abbott Spine, Austin, TX). Of these, the X STOP and the ExtenSure implants have been FDA approved for general use.33 The X STOP has an oblong central core that is stabilized by two lateral wings (Fig. 2-3). The primary indication is mild or moderate neurogenic claudication from spinal stenosis. For dynamic interspinous devices, the Diam (Medtronic Sofamor Danek, Memphis, TN), Coflex (Paradigm Spine, New York, NY), and CoRoent (Nuvasive Inc., San Diego, CA) have been investigationally studied for use in the United States.34 Of these, only the Diam device has been FDA approved. It attaches at the spinous processes and behind the supraspinous ligament. At the time of writing, numerous dorsal thoracolumbar dynamic systems have been approved by the FDA for investigational use. Outcome data for these systems, however, has been extremely limited.
Ventral Thoracolumbar Instrumentation
Successful use of the Harrington instrumentation kindled interest in developing a ventral system to address neuromuscular scoliosis. Dwyer developed a ventral system for internal fixation using screws connected by a cable.35 Winter attempted a combined ventral and dorsal approach with Harrington and Dwyer instrumentation to treat painful adult idiopathic scoliosis.36 This concept was of particular interest in that these patients were at high risk for pseudarthrosis and tended to tolerate bracing less well than adolescents.36
The Dunn device was a ventral implant that consisted of two rods that spanned the distance between two vertebral body bridges: one placed ventrolaterally with a vertebral body staple and the other placed more dorsolaterally with an intervertebral body screw.37 This system was not widely accepted because it was bulky and was associated with vascular complications.38
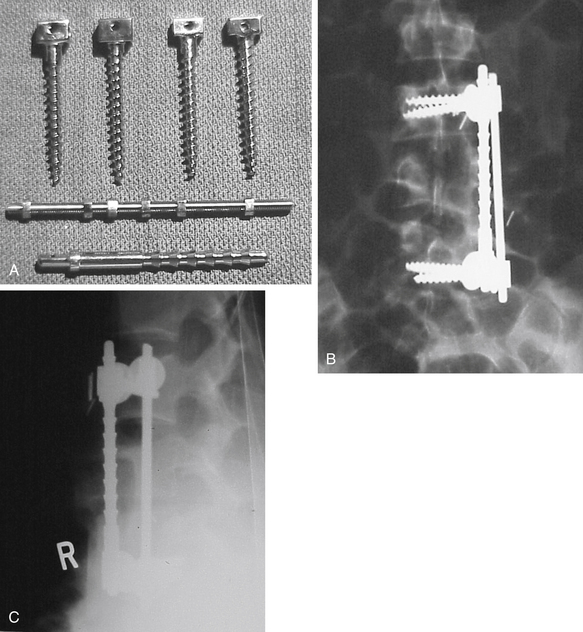
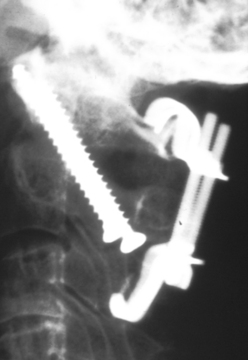
The ventral Kostuik-Harrington instrumentation was an adaptation of short Harrington rods used in conjunction with a pedicle screw developed by Paul Harrington for use in treating myelomeningocele. Introduced by John Kostuik in the early 1980s, it was an innovative short-segment ventral fixation device. The screw, when placed ventrolaterally in the vertebral bodies, allows for short-segment ventral correction of the kyphotic deformity associated with burst fractures. A second neutralization rod was placed parallel to the first rod to enhance stability (Fig. 2-4). Over time, cross-fixators were added in an attempt to further enhance stability. Two parallel rods rigidly cross-linked are the biomechanical equivalent of a plate. Most ventral short-segment constructs subsequently used plates with vertebral body screws.
Several other plate designs soon followed that had a lower profile. Ryan introduced a plate secured by a rostral and caudal bolt inserted through the vertebral body. The single-bolt design, however, offered less resistance to rotation than the designs that used two screws or bolts above and below.39 The Yuan I-Plate was an alternative design that consisted of a 3.5-mm stainless steel plate secured with transvertebral screws.40 Black et al.41 published their experience with a low-profile, rectangular, stainless steel plate with multiple holes that allowed for the placement of three screws at each vertebral level. The Kaneda device represented another stage in the development of ventral thoracolumbar instrumentation because it allowed reduction of kyphotic deformities after ventral decompression while providing good strength without incidence of vascular injury.38
Dorsal Cervical Instrumentation
Several instrumentation systems were devised as adjuncts or alternatives to wiring. The Daab plate was a stainless-steel implant shaped like an elongated H that could be compressed at either end to fixate it to a spinous process.42,43 This instrumentation represented no significant advantage over the available wiring techniques, and it was probably inferior, considering that it typically needed the resection of an intervening spinous process and the associated interspinous ligaments.
Halifax clamps are a pair of upgoing and downgoing sublaminar hooks tightened together with a screw that is then secured in position with a locking mechanism (Fig. 2-5).43,44 Halifax clamps have the advantage of relatively simple and rapid application. In addition, the area of bone contact is broader than that with wiring and is less likely to pull out of soft bone. They offer C1-2 fixation comparable to that achieved with the Brooks technique.45 Relative disadvantages of the system are that hooks are introduced into the spinal canal and the implant is relatively “high profile” and has limited application when stabilization is needed over multiple segments.
Related posts:
 Definition and Assessment of Dysfunctional Segmental Motion
Pathophysiology of Cervical Myelopathy: Biomechanics and Deformative Stress
Combined Ventral-Dorsal Surgery
Bone Void Fillers: Bone and Bone Substitutes
Medical Management of Neck and Low Back Pain
Posterior and Transforaminal Lumbar Interbody Fusion
Definition and Assessment of Dysfunctional Segmental Motion
Pathophysiology of Cervical Myelopathy: Biomechanics and Deformative Stress
Combined Ventral-Dorsal Surgery
Bone Void Fillers: Bone and Bone Substitutes
Medical Management of Neck and Low Back Pain
Posterior and Transforaminal Lumbar Interbody Fusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


