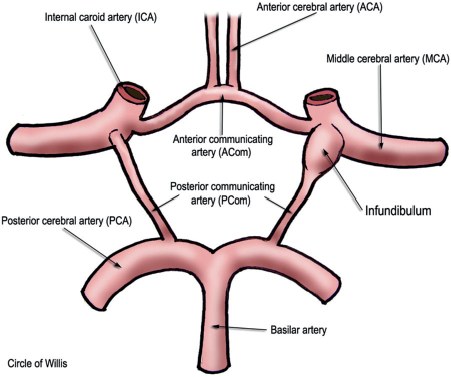
51 What features of intracranial vessels may make them more prone to aneurysm formation than extracranial vessels? • Fewer elastic fibers in the tunica media and adventitia1 • Less muscle in the media • Thinner adventitia • No external elastic lamina What is a saccular aneurysm? Bleb-like outpouching that arises in curves and bifurcations (sites of hemodynamic stress) of intracranial vessels; 90% arise in the anterior circulation2 What is an infundibulum? A funnel-shaped (pyramidal) dilation of a vessel’s origin with a vessel exiting at the apex of the funnel; most common at the PCom origin from ICA; detected in 5 to 17% of carotid arteriograms3 Fig. 51.1 Circle of Willis. In this representation we can see a left sided PCom infundibulum. An ovoid dilatation formed when damage to the arterial media (e.g., from infection, atherosclerosis, vasculitis) causes the vessel to dilate. Most common in the posterior circulation (vertebrobasilar) of older patients and often related to atherosclerosis. What is a mycotic aneurysm? An aneurysm formed when an infected embolus (e.g., bacteria, fungi) occludes the intima or vasa vasorum; most common intracranial location is the distal MCA What is a pseudoaneurysm? A tear through all three arterial layers with persistent flow outside of the vessel, usually due to a traumatic hematoma adjacent to the vessel (the “wall” of the aneurysm is formed by surrounding cerebral structures and contains no vascular elements) What is a common cause of intracranial pseudoaneurysm? Penetrating traumatic brain injury What is a “giant” aneurysm? An aneurysm >2.5 cm in size. The risk of rupture is very high, and early treatment is generally advocated. What are Charcot-Bouchard aneurysms? Microaneurysms occurring in small (<300 μm diameter) vessels primarily in the basal ganglia; associated with chronic hypertension What conditions are associated with aneurysms? • Female sex • Hypertension (HTN) • Atherosclerosis • Polycystic kidney disease (autosomal dominant; prevalence 10 to 30%)4 • Fibromuscular dysplasia • Vascular malformations (e.g., AVMs) • Collagen vascular disease (Ehlers-Danlos, Marfan) • Coarctation of the aorta • Neurofibromatosis-1 (NF1) • Family history of aneurysm What are the risk factors for aneurysm rupture? Cigarette smoking, HTN, large aneurysm size, young age, posterior circulation location, history of previous rupture from another aneurysm What is the most common presentation of a ruptured aneurysm? Subarachnoid hemorrhage (SAH) What is the risk of hemorrhage for an unruptured saccular aneurysm? Risk varies based on location and size, as shown in the following table5:
Intracranial Aneurysms
Size of unruptured aneurysm (mm) | 5-year rate of hemorrhage for anterior circulation aneurysm | 5-year rate of hemorrhage for posterior circulation aneurysm (including PCom) |
<7 | <0.01% | 2.5% |
7–12 | 2.5% | 14% |
13–24 | 14% | 18% |
>24 | 40% | 50% |
What are the mortality and morbidity associated with aneurysm rupture?
• 3-month mortality following aneurysmal SAH ranges from 50 to 60%6
• Risk of serious morbidity following SAH is 10 to 20%6
What are the other common forms of presentation of ruptured aneurysms?
• Intracerebral hemorrhage in 4 to 42.6%7,8
• Intraventricular hemorrhage (IVH) in 13 to 28%9 (IVH is often seen with distal PICA, ACom aneurysms, also seen rarely with basilar tip aneurysms)
What are the possible presentations of unruptured intracranial aneurysms?
• Minor hemorrhage (sentinel bleed)
• CN III palsy (in 9% of PCom aneurysms10
• Trigeminal neuralgia (usually in V1 or V2 distribution with intracavernous or supraclinoid aneurysms)
• Seizures
• Headache or migraines (retro-orbital)
• Visual loss (ophthalmic, ACom, basilar apex aneurysms)
• Endocrine disturbance (due to compression of pituitary stalk or gland by intrasellar or suprasellar aneurysms)
• Transient ischemic attacks or small infarcts (due to distal embolization)
• Incidental/asymptomatic
With which visual deficit are unruptured ophthalmic artery aneurysms classically associated?
Nasal quadrantanopsia
Which nonruptured presentation confers the greatest risk of imminent rupture?
Minor hemorrhage (sentinel bleed) has an average latency of only 11 days between symptom and clinically significant SAH.11
What other findings may indicate impending aneurysm rupture?
• Progressive cranial nerve (CN) palsy
• Increase in size of aneurysm on angiography
• “Beating aneurysm sign”: changes in aneurysm size between slices on imaging
The rupture of an aneurysm located on what artery may be the cause of an SAH in the following places: in the frontal horn?
Anterior choroidal
…in the interhemispheric fissure or gyrus rectus?
ACom
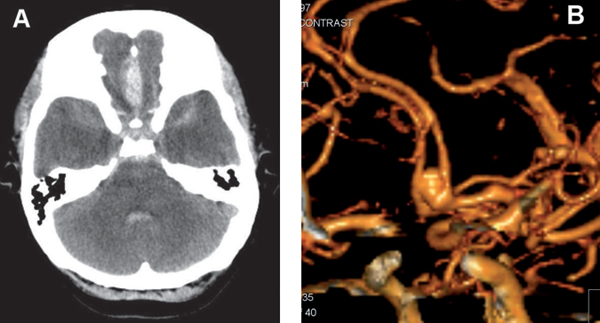
Fig. 51.2 (A) Axial CT scan revealing subarachnoid hemorrhage in the interhemispheric fissure. (B) CT angiogram correlate demonstrating the culprit: a 7-mm ACom aneurysm.







