Figure 91.1. Sequence of photographs showing involuntary movements in a patient with acute thalamic stroke, with flexion and external rotation of the lower limbs and eversion of both feet (myoclonic dystonia).
Involuntary motor phenomena with varied presentation have been reported in ischemic lesions of the brainstem. They can range from small amplitude movements similar to myoclonus to shaking of the limbs and even the trunk, which are often intermittent and can be triggered by painful stimuli. Their frequency is unknown, but they usually occur in extensive lesions of the brainstem usually related to acute basilar occlusion [16]. The pathophysiology is uncertain and the most likely is the corticospinal tract ischemia. Recognition of these movements, and consequent measures for quick diagnosis and treatment, are important because they may suggest the formation of a basilar occlusion.
91.9 Conclusions
In patients accessing the emergency room with a movement disorder of acute onset, clinical manifestations and etiology may be various. In such cases we must evaluate the autonomic disorders that may accompany the clinical features and establish the therapeutic measures that can sometimes require ICU admission (Figure 91.2).
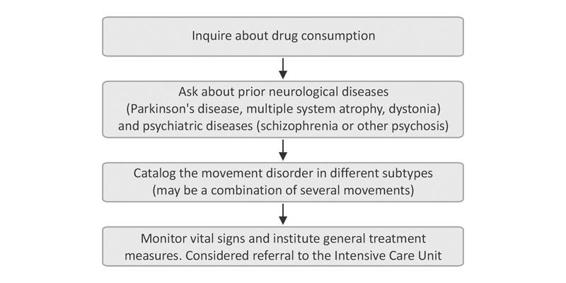
Figure 91.2. Algorithm for emergency management of acute movement disorders.
References
1. Kipps CM, Fung VSC, Grattan-Smith P, et al. Movement disorders emergencies. Movement disorders 2005; 20: 322-34
2. Poston KL, Frucht SJ. Movement disorders emergencies. J Neurol 2008; 255 (S4): 2-13
3. Linazasoro G, Van Blercom N. Síndrome neuroléptico maligno y catatonía letal. Neurol Suppl 2007; 3: 2-6
4. Admet P, Lestavet P, Krivosic-Horber R. Neuroleptic malignant syndrome. Br J Anaesth 2000; 83: 129-35
5. Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med 2005; 352; 11: 1112-20
6. Abraham RB, Adnet P, Glauber V. Malignant hyperthermia. Post Grad Med J 1998; 74: 11-7
7. Meinck HM, Thompson PD. Stiff man syndrome and related conditions. Mov Disord 2002; 17: 853-66
8. Serrano-Dueñas M. Neuroleptic malignant syndrome-like, or (dopaminergic malignant syndrome) due to levodopa therapy withdrawal. Clinical features in 11 patients. Parkinsonism Relat Disord 2003; 9: 175-8
9. Aarsland D, Larsen JP, Cummings JL, et al. Prevalence and clinical correlates of psychotic symptoms in Parkinson disease: a community-based study. Arch Neurol 1999; 56: 595-601
10. Vallderiola F, Pilleri M, Tolosa E, et al. Bilateral subthalamic stimulation monotherapy in advanced Parkinson’s disease: long-term follow-up of patients. Mov Disord 2002; 17: 125-32
11. Erro ME, Muñoz R, Zandio B, Mayor S. Acute parkinsonism after the accidental oral intake of mancozeb. Mov Disord 2011; 26: 557-8
12. Grandas F, Contreras A. Urgencias en distonía. Neurol Suppl 2007; 3: 35-9
13. Corominas Sánchez M, Lleonart Bellfill R, Pujol Farriols R. Acute laryngeal dystonia due to clebopride simulating allergic reaction. Med Clin (Barc) 2007; 129: 238-9
14. Dalmau J, Lancaster E, Martínez-Hernández E, et al. Clinical experience and laboratory investigations in patients with anti-NMDAR encephalitis. Lancet Neurol 2011; 10: 63-74
15. Erro ME, Navarro MC. Último minuto en trastornos del movimiento: Mioclonías. Revista de Neurología 2009; 48: S1-6
16. Herrera M, Erro ME, Aymerich N, et al. Movimientos involuntarios en lesiones isquémicas del tronco cerebral. Neurología 2007; 22: 475-9
Related posts:
 Acute Renal Injury in the Neurocritical Patient
Neurocritical Care of Patients With Arteriovenous Malformations
The Diagnosis and Management of Central Nervous System Infections in the Neurocritical Care Unit
Stroke Units: Organization, Past, Present and Future
Gastrointestinal Disorders in the Neurocritical Patient
Concepts and Management of Brain Death and Management of Potential Organ Donation
Acute Renal Injury in the Neurocritical Patient
Neurocritical Care of Patients With Arteriovenous Malformations
The Diagnosis and Management of Central Nervous System Infections in the Neurocritical Care Unit
Stroke Units: Organization, Past, Present and Future
Gastrointestinal Disorders in the Neurocritical Patient
Concepts and Management of Brain Death and Management of Potential Organ Donation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


