Chapter 13 Medial Branch Blocks
Cervical, Thoracic, and Lumbar

 Findings on radiographs, computed tomography, and magnetic resonance imaging are often inconclusive.
Findings on radiographs, computed tomography, and magnetic resonance imaging are often inconclusive.


 It is vital to realize the innervation of the facet joints as the facet joints receive dual innervation from two spinal nerves.
It is vital to realize the innervation of the facet joints as the facet joints receive dual innervation from two spinal nerves.
Establishing a Diagnosis
History and Physical Examination
History and physical examination are important for exclusion of other causes of spinal pain. On reviewing the medical history, several conditions can affect the facet joints. These include osteoarthritis, inflammatory arthritides (rheumatoid arthritis, ankylosing spondylitis, and reactive arthritis), synovial impingement, meniscoid entrapment, chondromalacia facetae, pseudogout, synovial inflammation, and villonodular synovitis,1–4 Signs on clinical examination that may point to facet pain include tenderness over the facet joints on palpation; pain that is characterized as deep, dull, and aching; pain that is difficult to localize; and stiffness, especially in the morning. Sudden onset of pain noted with twisting, bending, or rotary movements and pain aggravated on extension and lateral bending more than flexion are also consistent with facet joint–mediated pain, although the latter finding is unreliable. Additional physical examination findings may include muscle spasm and either hypalgesia or hyperalgesia over the area of pain. Flexion, extension, and rotation may or may not be decreased. The straight-leg raise results are usually negative. Given all of the above, the clinical criteria for facet joint–mediated pain are generally nonspecific and unreliable.5–7 Most maneuvers used in physical examinations are likely to stress several structures simultaneously, especially the discs, muscles, and facet joints, thus failing to provide any reasonable diagnostic criteria based on physical examination.
As stated previously, history and physical examination, along with radiologic imaging, cannot reliably be used to diagnose painful zygapophyseal joints. Therefore, medical branch blocks are needed to diagnose facetogenic pain.8 Numerous studies have tried to predict who will respond to facet joint injections. Revel et al9 identified seven variables associated with a positive response to facet joint injections: age older than 65 years, pain that was not exacerbated by coughing, pain not worsened by hyperextension, pain not worsened by forward flexion, pain not worsened when rising from flexion, pain not worsened by extension-rotation, and pain well relieved by recumbency. A later study by Revel et al10 found the presence of five among seven variables distinguished 92% of the patients responding to lidocaine injection and 80% of those not responding to lidocaine. However, further investigations of Revel et al’s variables by other investigators have been proven wrong.5
Injections in Facilitating the Diagnosis
Facet joint–mediated pain can be diagnosed with placebo-controlled or controlled local anesthetic diagnostic blocks using either facet joint blocks or medial branch blocks. The choice of technique used should be based on evidence of effectiveness of diagnosis and ease of technique. Evidence for diagnostic medial branch blocks using 80% pain relief with controlled diagnosed blocks are noted to be Level I or II-1 based on U.S. Preventive Services Task Force criteria.11,12 Medial branch blocks are relatively easier to perform and safer than intraarticular blocks because medial branch blocks can be performed even with osteophyte formation, which prevents entry into the facet joint. Additionally, the target area of the medial branch prevents overpenetration of the needle into the spinal canal during placement, therefore decreasing the possibility that the needle will pass through the target and into the spinal canal and cord, which can occur during intraarticular injections. Medial branch blocks also have therapeutic validity, but the therapeutic validity of intraarticular injection is lacking.11
False-positive rates of single local anesthetic blocks are high, ranging from 27% to 63% for cervical, 42% to 58% for thoracic, and 21% to 33% for lumbar medial branch blocks.12–14
Because of high false-positive rate of single local anesthetic blocks, numerous experts advocate performing diagnostic double blocks with either saline control or two different local anesthetics. Control blocks using normal saline under double-blind conditions is the most rigorous form of control blocks, requiring three blocks of the same joint. The first block would have to be with the local anesthetic to establish prima facie that the joint is symptomatic. To maintain the controlling effect of change and blinding, the second block would have to be either normal saline or inactive agent, and the third block would need to be the reciprocal agent.8 Despite this evidence, in a systematic study of the cost-effectiveness of using controlled facet blocks, Bogduk and Holmes15 determined that the use of placebo-controlled injections cannot be justified in the United States based on financial considerations.
In clinical practice, controlled diagnostic blocks with two local anesthetics with different durations are used. A true-positive response is one in which the patient reports complete relief of pain for a shorter duration when short-acting local anesthetic is used and a longer duration when a long-acting agent is used.16 Lidocaine 1% to 2% commonly used for the first block with a positive response is followed by a later block with bupivacaine 0.25% to 0.5% 2 to 4 weeks later.11,17 Response patterns of medial branch blocks using bupivacaine and lidocaine were defined by Barnsley et al.16
A concordant response confirms that the joint is the source of pain with confidence of 85%.18
Anatomy
The Facet Joint
The basic anatomical unit of the spine is referred to as a three-joint complex that consists of paired zygapophyseal joints and an intervertebral disc (Fig. 13-1).19 This articular triad functions to stabilize and support the spine along with limiting motion of the spine.
The term zygapophyseal joint (or facet joint) originated from the Greek root zygos, meaning yoke or bridge, and physis, meaning outgrowth. Therefore, the facet joints bridge the vertebrae behind the vertebral foramina.20 Facet joints are paired diarthrodial synovial joints formed by inferior articular process of one vertebra and superior articular process of the subjacent vertebra. Facet joints share the same general characteristics of synovial joints. As true synovial joints, each facet joint contains distinct joint space capable of accommodating 1 to 1.5 mL of fluid, a synovial membrane, hyaline cartilage surfaces, and fibrous capsule. The fibrous capsule of the facet joint is composed mostly of collagenous tissue arranged more or less in transverse fashion to provide maximum resistance to flexion. The thick fibrous joint capsule is covered by synovial membrane superiorly, posteriorly, and inferiorly. Anteriorly, the synovial membrane lacks a true fibrous capsule and instead is in direct contact with the ligamentum flavum.19
Facet joints are richly innervated with three types of nerve endings: encapsulated (Ruffini-type endings, pacinian corpuscles), unencapsulated, and free nerve endings.19 The presence of low-threshold, rapidly adapting mechanosensitive neurons lining the facet capsule suggests that in addition to transmitting nociceptive information, the facet capsule also serves proprioceptive function.21,22
Facet capsule nerve endings contain substance P, calcitonin gene-related peptide, and neuropeptide Y.23,24 Inflammatory mediators such as prostaglandins, inflammatory cytokinase, interleukin 1B, interleukin 7, and tumor necrosis factor have also been found in facet joint cartilage and synovial tissue.25,26
The orientation of the facet joints varies at the cervical, thoracic, and lumbar regions. Facet joints oriented parallel to the sagittal plane provide substantial resistance to axial rotation but minimal resistance to shearing forces (backward and forward sliding), and facet joints oriented more in a coronal plane tend to protect against flexion and shearing forces but provide minimal protection against rotation. The cervical facets are orientated in a coronal plane, which allows for flexion, extension, and lateral bending. The C2-C3 to C5-C6 facets are angled 35 degrees from the coronal plane, and C7-T1 are angled 22 degrees from the coronal plane. Orientation of the C5-C6 facet joint is between 22 and 35 degrees. All cervical facet joints from C2-C3 to C7-T1 are angled 110 degrees from the midline posterior sagittal plane. In the cervical spine, it is important to remember that the vertebral artery passes through the foramen of the transverse process of C1-C6.27
Facet joints in the thoracic spine differ from that of the cervical and lumbar spines in that their orientation is in a more coronal direction, which allows thoracic facet joints to play an important role in stabilization of thoracic spine during flexion loading. The T1-T2 facet joint is angled 66 degrees from a transverse plane, with the cephalad end more anterior than the caudad end. The T3-4 to T11-T12 facet joints are angled 75 degrees from the transverse plane. The T1-T2 to the T11-T12 facet joints are uniformly angled 110 degrees from the midline posterior sagittal plane. The T12-L1 facet joint is 25 degrees oblique to the sagittal plane from the midline posteriorly, which is similar to the lumbar orientation.28,29
The upper lumbar facet joints (T12-L2) are oriented closer to the midsagittal plane of the vertebral body, which allows limited rotational movements and favors flexion and extension. The lower facet joints tend to be oriented in a more coronal angle, which allows for greater rotational movements. The lumbar facet joints’ cephalad ends are farther anterior than the caudad ends because the facet joints are tipped approximately 10 degrees. In the upper lumbar spine, approximately 80% of the facet joints are curved, and 20% are flat; in the lower lumbar spine, these numbers are reversed.30,31 The lumbar facet joints transition from a coronal orientation to a sagittal positioning with age. Some studies have shown a positive association between degenerative spondylolisthesis and more sagitally oriented lower lumbar facet joints.32
Innervation
Cervical
The facet joints are innervated by the dual nerve supply from the medial branch of the dorsal ramus. Cervical facet joints from C3-C4 to C7-T1 are supplied by medial branches from the same level and the level above. Medial branch nerves arise from the posterior primary rami located in the cervical intertransverse space and then passes dorsally and medially to wrap around the waist of the articular pillar. The location of this nerve on the articular pillar is essentially the same as those of nerves C4-C8. The medial branches are bound to the periosteum by an investing fascia and are held against the articular pillars by tendons of the semispinalis capitis. The C7 medial branch crosses the root of the C7 transverse process and therefore lies higher on the lateral projection of the C7 articular pillar.33
The C2-C3 facet joint differs in innervation in that their innervation comes from the third occipital nerve along with C2 and C3 medial branches. Two medial branches usually arise separately from the C3 dorsal ramus. The superior and larger branch is the third occipital nerve (also known as the superficial medial branch), and the inferior branch is the deep medial branch. The third occipital nerve innervates C2-C3 joint. It curves dorsally and medially around the superior articular process of the C3 vertebra and crosses the C2-C3 facet joint either just below or across the joint margin. It also provides cutaneous neural supply for the suboccipital region. The C3 dorsal ramus is the only cervical dorsal ramus below C2 that has a cutaneous distribution.34,35
The C8 medial branch runs a course similar to the upper thoracic nerves. It arises from the dorsal ramus within lateral margin of the intervertebral foramen of C7-T1. Because of the C8 medial branch and seven cervical vertebrae, numbering of medial branches is different in the cervical region compared with in the thoracic and lumbar spine. The facet joint is innervated by a cervical medial branch at the same level and level above for C4-C7. For example, the C5-C6 facet joint is innervated by the medial branches of C5 and C6. This numbering applies to the C4 through C7 levels.34,36
Thoracic Innervation
The course of the medial branches of T11 and T12 also vary because of different osseous anatomy at these levels. The T12 transverse process is shorter compared with other levels. Therefore, the T11 branch runs across the lateral surface of the root of the relatively short T12 transverse process. At the T12 level, the medial branch assumes a course analogous to those of the lumbar medial branches.28,37,38
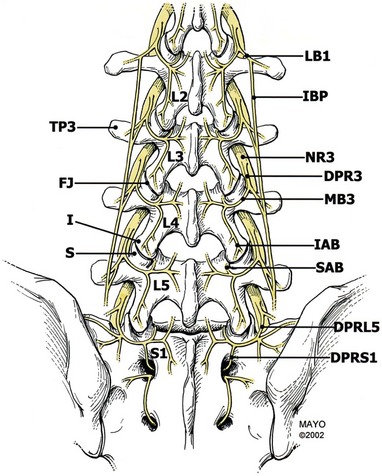
Lumbar Innervation
The primary dorsal rami divide into three nerves as they approach their respective transverse processes: the medial branch, intermediate branch, and lateral branch. The medial branch is the largest of the dorsal branch nerves. The medial branch has three branches as well. The proximal branch hooks around the articular process to supply the facet above. The medial descending branch passes medially and downward to innervate the superior and medial portions of the facet capsule below, the multifidus and interspinales muscles and ligament, and the periosteum of the neural arch. The ascending branch supplies the facet above. The other two main branches of the dorsal ramus are the intermediate branch and the lateral branch. The intermediate branch sends fibers into the longissimus muscles. The lateral branch innervates the iliocostalis muscle, the thoracolumbar fascia, the skin of the lower back and buttock, and the sacroiliac joint, but does not innervate the facets.22,39
The medial branches of L1-L4 rami have a predictable course. These medial branches come off the dorsal ramus and exit from the intervertebral foramen, piercing the intertransverse ligament and crossing the superior border of the transverse process. The branches then travel along the junction of the transverse process and superior articular process. This junction is often referred to as a “groove.” The medial branch nerve runs in the groove along the lateral aspect of the neck of the superior articular process, traveling caudally and posteriorly where it is in direct contact with the base of the superior surface of the transverse process, passing under the mamilloaccessory ligament. At L3, L4, and L5 levels, this ligament can become calcified. The medial branch nerve then proceeds inferiorly and posteriorly, where it sends fibers cephalad to innervate the caudad capsular margin of the adjacent superior joint capsule. Then it sends fibers to the next lower level at its cephalad capsular margin.20,40
The course of the L5 medial branch is somewhat modified because the transverse process is replaced by the ala of the sacrum. The L5 medial branch is not the medial branch of L5 but rather the dorsal primary ramus of L5, which is longer. The dorsal ramus pierces the intertransverse ligament and runs caudally and posteriorly along the groove formed by the junction of the superior articular process and sacral ala. The L5 dorsal ramus divides into two branches, a medial and lateral branch. The L5 medial branch curves medially around the base of the L5-S1 joint, sending an articular branch to this joint and then supplying the multifidus muscles. There is no mamilloaccessory ligament at this level. However, fibrous tissue fixes the position of the nerve at the base of the superior articular process. The lateral branch of the L5 dorsal ramus runs caudad to communicate with the S1 dorsal ramus lateral branch.41,42
Basic Science
Pain Referral Patterns
The distribution of referred pain appears to be related to the innervation of the medial and lateral branches of the dorsal rami. Studies of mapping out referral patterns have used asymptomatic volunteers and pain patients. Referral patterns from cervical zygapophyseal joints were studied by Dwyer et al.43 In their first study, the facet injections were done in normal volunteers, which showed certain referral patterns. The accuracy of referral patterns were later studied on symptomatic patients. Referral patterns obtained were C2-C3 as pain located in the upper cervical region and extending at least onto the occiput. The C3-C4 pattern is located over the posterolateral cervical region without substantial extension into the occiput and extending caudally over the posterolateral aspect of the neck without entering the region of the shoulder girdle. The C3-C4 pattern basically covers the area that is coextensive with the underlying levator scapulae muscle. Whereas the C4-C5 pattern is concentrated over the angle formed by the top of the shoulder and side of the neck, the C5-C6 pattern spreads laterally toward the shoulder with the main area draping over the top, front, and back of the shoulder girdle, with a base coinciding with the spine of the scapula. The C6-C7 pattern extends below the spine of the scapula. The typical C7-T1 pain pattern extends into the paravertebral area with coverage over the scapulae.44
The thoracic facets may produce middle back pain that is paraspinous with neuralgic characteristics. Thoracic referral patterns were noted by joint distention in normal volunteers. Some overlap was noted in the thoracic area. The pain was usually one to two segments inferior and lateral to the involved joint and unilateral. The T1-T2 joint pain was noted to be below the inferior angle of the scapulae. Despite this, there is a wide overlap in thoracic referral patterns that makes them unreliable.44–46
Referred pain from the lumbar zygapophyseal joints and medial branches has been examined in numerous studies showing overlap of referred pain between each level.47,48 Pain from L1-L3 has been shown to extend into the flank, hip, and upper lateral thighs. Pain from L3-S1 has been shown to extend deeper into the thigh, usually laterally and posteriorly and also into the groin area. Referred pain from the L4-5 and L5-S1 facet joints can also cause pain extending into the lower lateral leg, below the knee, and even to the foot at times.20,47,49 Referred pain may also assume a pseudoradicular pattern, making the underlying diagnosis difficult to confirm based on pain patterns.50




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


