Chapter 110 Metabolic Bone Disease
Beyond immediate surgical concerns, medical evaluation and treatment of the underlying metabolic bone disease is crucial to a successful long-term outcome. For many patients, the presenting symptom of previously unrecognized and untreated osteoporosis is a painful vertebral fragility fracture. Unfortunately, the majority of patients who have experienced a fracture do not receive appropriate treatment for osteoporosis. Approximately 50% of female patients who have sustained a compression fracture do not receive osteoporosis treatment.1 The rate of treatment after fracture is even lower for men. A recent retrospective study of 1171 men aged 65 or older demonstrated that only 7.1% of osteoporotic subjects and 16.1% of those with a hip or vertebral fracture received medication for osteoporosis.2 This represents a significant missed opportunity to reduce the risk of future fractures, particularly since the likelihood of refracture approaches 10% to 20% within 1 year of the initial fracture.
Osteoporosis
Definition
Osteoporosis is defined as “systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue with a consequent increase in bone fragility and susceptibility to fracture.”3 Although the diagnosis of osteoporosis in asymptomatic individuals is typically based on bone density measurement alone, this definition emphasizes the important role of unmeasured ultrastructural abnormalities that contribute to the clinical end point of fracture. In fact, the incidence of hip fracture increases between the ages of 50 to 90 years seven times more than predicted on the basis of decline in bone density alone.4
Prevalence and Costs
The prevalence of osteoporosis increases with age in both men and women. It is estimated that currently about 10 million Americans older than 50 years of age have osteoporosis.5 This number is expected to increase to more than 14 million people in 2020.6 Though osteoporosis is commonly conceived of as a disease of women, more than 30% of people with osteoporosis are men. The clinical consequence of osteoporosis is fracture. The 2004 U.S. Surgeon General’s report on Bone Health and Osteoporosis concluded that osteoporosis results in approximately 1.5 million fragility fractures annually. Vertebral compression fractures are the most common, accounting for about 700,000 fractures per year. More than 50% of women and 30% of men will experience a vertebral compression in their lifetime. As many as 20% of people who suffer from a vertebral fragility fracture will experience another within 1 year.5
Beyond the personal suffering and functional impact, the economic burden to society of osteoporosis is considerable. The estimated cost of caring for the greater than 2 million osteoporotic fractures in 2005 was estimated to be $17 billion.6,7 These figures are expect to increase by 50% by 2025, when the annual fracture incidence will surpass 3 million and costs will exceed $25 billion. A significant portion of this anticipated increase is a result of the growing problem of osteoporosis in the Hispanic population.6
Pathophysiology
Peak bone mass is achieved by about age 30 years in both sexes. Differences in peak bone mass account for some of the variation in osteoporosis risk between men and women as well as between racial and ethnic groups. For example, African American women have higher bone densities than non-Hispanic women at all ages and are at lower risk for fractures of the spine and hip.8 Since achievement of genetically determined peak bone mass occurs primarily before the age of 20 years, osteoporosis in later life may, in part, be regarded as a pediatric disease with geriatric consequences.9 Juvenile calcium intake is positively associated with bone mass in the fourth decade of life.10
Age-related bone loss begins in the fourth decade and continues throughout life in men and women. By the eighth or ninth decade of life, women have lost approximately 35% of their cortical bone mass and 50% of their trabecular bone mass.11 Men lose about 60% as much during their lifetimes. Menopause in women is associated with a period of accelerated loss of trabecular bone that persists for about 10 years. Thereafter, bone loss from trabecular and cortical sites continues at a slower rate, similar to that of men. Skeletal sites that are predominantly trabecular in composition, including vertebral bodies and distal forearm bones, are therefore at greatest risk for earlier osteoporosis. Rates of Colles and vertebral fractures in women rise sharply after menopause.12
The major cause of primary age-related osteoporosis in both men and women is loss of gonadal function. In young adults, skeletal remodeling is an ongoing process with closely coupled bone resorption and formation. In estrogen-deficient women, bone resorption as assessed by biochemical markers increases by 90%, while bone formation markers increase only 45%, reflecting an imbalance between bone formation and resorption with net bone loss.12 Estrogen has multiple effects on both osteoclast and osteoblast function. Estrogen suppresses osteoclast development by suppressing RANKL production as well as regulating production of osteolytic cytokines including interleukin-1, interleukin-6, tumor necrosis factor alpha, and prostaglandins.12,13 Estrogen plays a role in bone formation by stimulating production of growth factors by osteoblasts.14 The principal risk factors for primary osteoporosis in women are related to estrogen deficiency: postmenopausal status; nulliparity; late menarche; early menopause (before age 45), either natural or surgical; and secondary amenorrhea related to exercise or eating disorders. As in women, estrogen plays a critical and dominant role in maintaining bone density in men. While androgens are important determinants of muscle mass in males, serum estradiol levels are more predictive of bone density. Peripheral aromatization of androgens to estrogen is important in maintaining estradiol levels above the threshold required to maintain skeletal homeostasis.2
In older men and women, other factors contribute to age-related bone loss, including physiologic hyperparathyroidism, vitamin D deficiency, and secretion of various bone-resorbing cytokines.7,12 Recent studies suggest a remarkably high level of vitamin D deficiency among older adults. In a recent study, more than 50% of older North American women currently treated for osteoporosis were found to have suboptimal vitamin D levels.15 In the patients with fractures or falls, the prevalence of vitamin D deficiency exceeds 90%.16 In most studies of older adults, the prevalence of low serum vitamin D levels is unrelated to gender, race, latitude, or global location.17
Risk Assessment
In addition to the changes in bone density related to decline in gonadal function in both men and women, multiple lifestyle factors, medical disorders, and drugs may exacerbate or accelerate “age-related” bone loss (Box 110-1).18 Approximately 50% of men with osteoporosis have underlying “secondary” causes, and as many as one third of women with osteoporosis are found to have other conditions beyond estrogen deficiency.2,19,20 In men with osteoporosis, the most common secondary causes are hypogonadism, glucocorticoid use, and alcoholism. In women, secondary causes are more common in perimenopausal women and include glucocorticoid use, thyroid hormone excess, hypoestrogenemia, and anticonvulsant treatment.18
Measurements of bone mineral density alone are insensitive as predictors of risk of clinical fragility fractures. More than 90% of these fractures occur in individuals who do not have osteoporosis as defined by bone density measurement criteria.21 Incorporating assessment of clinical risk factors for bone loss and fracture risk into predictive models for fragility fracture, with or without bone mineral density measurement, greatly enhances the assessment of fracture risk in both men and women.22 The World Health Organization (WHO) has developed such a fracture risk assessment tool (FRAX), which incorporates multiple risk factors including body mass index, personal history of previous fracture, history of parental hip fracture, current smoking, history of long-term glucocorticoid use, rheumatoid arthritis, and daily alcohol consumption of three or more units.23 The tool also includes the presence or absence of other secondary causes of osteoporosis, including hypogonadism, inflammatory bowel disease, prolonged immobility, organ transplantation, type 1 diabetes, and thyroid disorders. FRAX is available to clinicians online (www.shef.ac.uk/FRAX) and provides estimates of the 10-year probability of hip fracture and major osteoporotic fracture.
Morbidity and Mortality
Osteoporosis is similar to hypertension as a disorder with a long asymptomatic interval before resulting in clinical manifestation. If unrecognized and untreated in its preclinical phase, osteoporosis may result in significant morbidity and mortality. Fragility fractures are the single most morbid and clinically significant consequence of osteoporosis, occurring most frequently in the vertebral body, proximal femur, and distal radius.5
The presence of a vertebral fracture, even if asymptomatic, increases the risk of future vertebral fracture fivefold and doubles the risk of hip fracture.1 In addition, these patients may experience chronic low back pain, loss of height, and kyphosis, leading to symptomatic biomechanical changes in the spine.7 Pulmonary compromise may become evident as a result of the kyphosis and compression fractures manifested by restrictive lung disease with decreased vital capacity.24 On average, each thoracic vertebral fracture reduces pulmonary vital capacity by 9%.24,25 In addition, shortening of the thoracic spine may result in compression of the abdominal contents, resulting in symptoms of early satiety and bloating. This may result in anorexia and weight loss, which is a great concern in a population of individuals who are already frail.
Patients with compression fractures also experience lower levels of functional performance compared with controls, including difficulty with performance of activities of daily living. These patients may become more sedentary as a result, with progressive deconditioning and further bone loss. The constellation of the preceding symptoms, as well as low self-esteem due to body image changes, may result in depression in up to 40% of individuals with osteoporosis. Patients who are at greater likelihood of developing depression are those with more than one compression fracture, those who are older, and those who are more socially isolated.24
Patients with a compression fracture were found to have a 23% higher age-adjusted mortality rate in a recent prospective cohort study of almost 10,000 women age 65 years or older.26 The mortality rate is even greater in patients with hip fractures, reaching 20% more than age-matched controls in the first year after hip fracture.7 Increased mortality after hip fracture is usually due to coexisting illness or deep venous thrombosis with pulmonary embolism from the relative immobilization associated with the fracture.27 Patients who survive the hip fracture often have limited ability to perform activities of daily living and require prolonged institutional care. In individuals over 75 years of age, hip fracture mortality is greater in men than in women: 20.7% and 7.5%, respectively.2,6
Diagnosis of Osteoporosis
A painful fracture is the most obvious clinical consequence of osteoporosis, but as many as 70% of osteoporotic spine fractures are asymptomatic.28 While a clinical diagnosis of osteoporosis may be made in the presence of a fragility fracture in the absence of bone mineral density measurement, low bone mass is recognized as a more sensitive diagnostic parameter in the absence of symptoms.29 Low bone mass is also a strong predictor of future fracture risk. The WHO has defined osteoporosis and osteopenia on the basis of bone mineral density (BMD) (Table 110-1). A T score is defined as the number of standard deviations above or below the average BMD for healthy young white females. The Z score is defined as the number of standard deviations above or below the average BMD for age- and sex-matched controls. Osteoporosis is present when the T score is at least −2.5. Severe osteoporosis is defined as a T score of at least −2.5 in the presence of one or more fragility fractures. Z scores are used preferentially to assess bone loss in premenopausal women and males younger than 50 years of age. A low Z score (<−2.0) represents bone loss in excess of age-expected loss and suggests that secondary causes of bone loss may be present.18,30 The WHO thresholds were chosen on the basis of fracture risk in postmenopausal Caucasian women. Similar diagnostic threshold values for men are less well defined. However, several studies have demonstrated that the age-adjusted fracture risk for any given BMD is similar in men and women.31 The International Society for Clinical Densitometry (ISCD) advises that the WHO criteria be used in postmenopausal women and in men age 50 and older but not in premenopausal women or men less than 50 years old, as the fracture risk is not the same in younger men and women.
TABLE 110-1 Osteoporosis and Osteopenia: World Health Organization Criteria
| Classification | Criteria |
|---|---|
| Normal | BMD up to ±1 SD of the main of the young adult reference range |
| Osteopenia | BMD between 1 and 2.5 SD below the main of the young adult reference range |
| Osteoporosis | BMD greater than 2.5 SD below the mean of the young adult reference range |
| Severe osteoporosis | BMD greater than 2.5 SD below the mean of the young adult reference range in the presence of one or more insufficiency fractures |
BMD, bone mineral density; SD, standard deviation.
Several technologies are available to measure bone mass, including forearm single-photon absorptiometry, spine and hip dual-photon absorptiometry, and quantitative ultrasound of the calacaneus. While multiple studies have shown that these various measurement techniques may predict osteoporotic risk,32–37 the gold standard remains dual-energy x-ray absorptiometry (DEXA) of the hip and spine for the diagnosis of osteoporosis.8,18,30 DEXA is considered the gold standard because it has been shown to be precise (1%–2%) and to have acceptable accuracy and good reproducibility. It is also the most extensively validated test for fracture outcomes.29,30 Other advantages of DEXA include relatively low radiation exposure, wide availability, and the capacity to measure bone density at multiple skeletal sites. The ISCD recommends obtaining BMD measurements of the spine and hip. Numerous studies have shown that BMD measured at the femur (neck or total hip) is the best for predicting hip fracture risk.3,30,31,38 Spinal BMD is the optimum for monitoring response to treatment. The risk of hip fracture is increased 2.6 times for each standard deviation decrease at the femoral neck.31,39 Serial BMD measurements should be performed on the same machine for the same patient, owing to variability of BMD assessment between machines of different manufacturers.
Most clinical guidelines recommend screening healthy women for osteoporosis at age 65 and testing higher-risk women earlier. The ISCD recommends screening men without risk factors for osteoporosis at age 70 and testing higher-risk men earlier. Risk factors are as noted previously. Another indication for screening is radiographic evidence of osteopenia or vertebral fracture.30 In addition, screening is recommended for people who have diseases associated with bone loss, such as rheumatoid arthritis, as well as people initiating long-term corticosteroid therapy. Current evidence does not support routine screening of all perimenopausal women, as its value in directing preventive therapy against future fractures has not been established8 (Box 110-2).
BOX 110-2 Osteoporosis Screening Guidelines
• Women age 65 and older, men age 70 and older (regardless of clinical risk factors)
• Younger postmenopausal women and men ages 50 to 69 for whom there may be concern based on their clinical profile
• Women in menopausal transition who may have a risk factor for increased fracture (low body weight, high-risk medication, or prior low trauma fracture)
• Adults who sustain a fracture after age 50
• Adults taking glucocorticoids in a daily dose of ≥5 mg or equivalent for 3 months or more
• Any person being considered for pharmacologic therapy for osteoporosis
• Anyone being treated with osteoporosis to monitor effect (generally every 2 years)
• Anyone not receiving therapy in whom evidence of bone loss would lead to treatment
Bone turnover markers reflecting bone formation and resorptive activity are not recommended for routine diagnostic purposes, as they have not been found to predict bone mass or fracture risk. Indices of bone formation include alkaline phosphatase and osteocalcin. Markers for resorption include serum and urine levels of type I collagen C- and N-telopeptides. While not reliable diagnostically, they have been found helpful in clinical trials in understanding the mechanism of bone loss. Bone markers may also be helpful for monitoring response to therapy and compliance.8
Evaluation of patients with osteoporosis should include a thorough history and physical examination, as most of the secondary causes of osteoporosis can be excluded with a careful history and physical examination. A minimum screening laboratory profile should be considered for all patients who have been diagnosed with osteoporosis. This is particularly important in men, as 30% to 60% will have an identifiable secondary cause. Approximately 50% of perimenopausal women with osteoporosis also have a secondary cause, including hypoestrogenemia, glucocorticoid usage, thyroid hormone excess, and anticonvulsant therapy.18 As was mentioned previously, patients with an abnormal Z score should also be studied more aggressively for secondary causes. Initial general screening should include a complete blood count, erythrocyte sedimentation rate, serum calcium, serum 25 hydroxyvitamin D, phosphorus, alkaline phosphatase, creatinine, aspartate aminotransferase, thyroid-stimulating hormone (TSH), and serum protein electrophoresis. Tannenbaum et al. looked at the yield of laboratory testing to identify secondary causes of osteoporosis in otherwise healthy women. Their findings suggest that a basic screen of serum calcium, serum parathyroid hormone (PTH), and 24-hour urinary calcium excretion in all patients, and a serum TSH in patients on thyroid replacement, provides a high diagnostic yield (86% in their study) at a low cost (mean cost of $75/patient).40 In male patients, serum testosterone should be obtained. Additional studies such as 24-hour urinary calcium, PTH, and serum immunoelectrophoresis should be obtained selectively on the basis of risk factors and preliminary studies (Table 110-2).
TABLE 110-2 Screening Laboratory Tests
| Test | Purpose |
|---|---|
| CBC | Evaluate for bone marrow malignancy, infiltrative process, or malabsorption |
| Serum calcium | Decreased in those with malabsorption or vitamin D deficiency, increased in hyperparathyroidism |
| Liver function | Evaluate for intrinsic liver abnormality |
| Alkaline phosphatase | Increased in acute fractures, prolonged immobilization, and Paget disease of the bone |
| TSH | Screen for hyperthyroidism |
| ESR | May indicate an inflammatory process or monoclonal gammopathy (associated with bone loss) |
| Serum 25-hydroxyvitamin D | Evaluate for vitamin D deficiency |
| Serum calcium | Decreased in those with malabsorption or vitamin D deficiency, increased in hyperparathyroidism |
| Serum phosphorus | Decreased in patients with osteomalacia |
| PTH | Screening for hyperparathyroidism |
| Creatinine | Renal failure is associated with secondary hyperparathyroidism |
| Serum testosterone | In all men to screen for hypogonadism |
| Serum estradiol | Screening for hypogonadism in premenopausal or perimenopausal women |
| Urinary calcium excretion | 24-hour urinary excretion on a high-calcium-intake diet screens for malabsorption and hypercalciuria |
| SPEP/UPEP | If monoclonal gammopathy is suspected |
CBC, complete blood count; ESR, erythrocyte sedimentation rate; PTH, parathyroid hormone; SPEP/UPEP, serum protein electrophoresis/urine protein electrophoresis; TSH, thyroid-stimulating hormone.
Prevention of Osteoporosis
Because currently available treatments for established osteoporosis reduce fracture rates by 50% to 60% at best and restore only a small portion of skeletal bone, prevention of osteoporosis remains the ideal objective in maintaining skeletal health. Optimizing peak adult bone mass is crucial, as low peak adult bone mass is a major risk factor for subsequent development of osteoporosis. Although as much as 75% of peak adult bone mass is genetically determined, nutrition and physical activity play important roles in optimizing bone mass from infancy to adulthood.41
Hormone Replacement Therapy
Until the Women’s Health Initiative studies were reported in 2002 through 2004, perimenopausal women were typically considered for hormone replacement therapy to preserve bone and prevent the steep escalation in bone loss in the early postmenopausal years.42–44 Although this trial demonstrated a 34% reduction in hip and vertebral fractures in postmenopausal women treated with conjugated estrogens or estrogens plus progestin, other health risks, including coronary artery disease, stroke, and venous thromboembolism, exceeded benefits. Because of the unfavorable risk-to-benefit ratio and the availability of other effective nonhormonal drugs, hormone replacement therapy is not recommended for prevention of osteoporosis in women without vasomotor or other menopausal symptoms requiring treatment.
Nutrition
Lifelong adequate intake of calcium and vitamin D is essential to achieving peak bone mass and prevention of osteoporosis. Calcium supplementation has been shown to have a positive effect on accrual of bone mass throughout childhood and adolescence.45 Calcium supplementation has been shown to retard bone loss in postmenopausal women.46 For children ages 3 to 8 years, 800 mg of calcium per day is recommended.8 After age 8 and through adult life, most guidelines recommend a daily intake of 1200 to 1500 mg of calcium from both dietary and supplemental sources.8,47 Unfortunately, more than 50% of adolescents and young adults do not ingest sufficient dairy products to achieve dietary calcium requirements.8
Vitamin D plays an important role in optimal calcium absorption. Vitamin D adequacy has been defined as the level of vitamin D necessary to achieve maximal suppression of PTH, while avoiding the negative skeletal effects of secondary hyperparathyroidism.45 In adolescents, vitamin D levels correlate with bone mineral content, and the vitamin probably plays a crucial role in achieving peak bone mass.48 In older adults, a dose-response relationship between vitamin D and fracture reduction has been demonstrated, with a 20% reduction in hip fracture risk in individuals taking higher doses.49 As with calcium, the decrease in dairy product consumption, particularly of vitamin D enriched or fortified milk products, contributes to inadequate consumption of this vitamin. For adults, the National Osteoporosis Foundation recommends an intake of 800 to 1000 international units (IU) of vitamin D per day. The best measure of vitamin D status is the serum level of 25(OH)D. A 25(OH)Dlevel of greater than 32 ng/mL is the target that is considered optimal to achieve full suppression of PTH for osteoporosis prevention. The requirement for other micronutrients that are important in skeletal health, including magnesium, fluoride, vitamin C, vitamin K, and potassium, are easily met by a healthy diet that includes five servings daily of fruits and vegetables.45
Exercise
In prepubertal and peripubertal children, active weight-bearing exercise has been demonstrated to increase bone mineral density as measured by DEXA or calcaneal ultrasound.50,51 In premenopausal women, total weight-bearing physical activity correlates with bone density, the strongest association with physical activity being during early age periods.52 These studies suggest that early active, weight-bearing exercise is important in achieving peak adult bone mass. There is little evidence that exercise in midlife significantly increases BMD, however.8 In older patients, weight-bearing exercise slows bone loss but has not been shown to decrease fracture risk.53 However, regular exercise in older patients has been shown to reduce the risk of falls by about 25%, potentially reducing the risk of osteoporotic fracture.54 The National Osteoporosis Foundation strongly endorses lifelong physical activity at all ages, including weight-bearing exercise and muscle-strengthening exercise.
Who Should Be Treated?
Because osteoporosis, like hypertension, is a silent disease until it manifests clinically as fracture, screening for asymptomatic disease in high-risk individuals represents an initial step before treatment. BMD measurement by DEXA represents the screening tool of choice. As was noted earlier, the WHO has defined osteopenia and osteoporosis on the basis of this measurement. However, though fracture rates are highest in individuals with osteoporosis as defined by these criteria, more than 80% of postmenopausal women with fractures have T scores better than −2.5.55 Most fractures occur in patients with BMD in the range defined as osteopenia. However, pharmacologic treatment of women with osteopenia defined by BMD in the absence of other risk factors is not cost effective.56 Fracture risk depends not only on BMD values but also on other independent variables, including body mass index, age, history of prior fracture, parental history of hip fracture, glucocorticoid use, tendency to fall, poor mobility, and other secondary factors.57,58 The FRAX tool described previously represents one attempt to predict fracture risk by using a model that incorporates BMD and clinical risk factors.31 Although biochemical markers of bone remodeling have been shown to identify perimenopausal women who are at increased risk for rapid bone loss, the role of markers in predicting fracture risk and determining who should be treated is uncertain.59
Current guidelines recommend that pharmacologic treatment should be offered to men and women who have known osteoporosis and to those who have experienced fragility fractures.47,60 Both the American College of Physicians and the National Osteoporosis Foundation recommend that clinicians consider pharmacologic treatment for men and women who are at increased risk for developing osteoporosis based on a analysis of risk factors. The National Osteoporosis Foundation specifically defines this population with a 10-year probability of a hip fracture greater than 3% or a 10-year risk of a major osteoporotic fracture greater than 20% based on the FRAX calculator.
Pharmacologic Therapy
Pharmacologic therapy for the treatment of osteoporosis can be classified as antiresorptive or anabolic (Table 110-3).
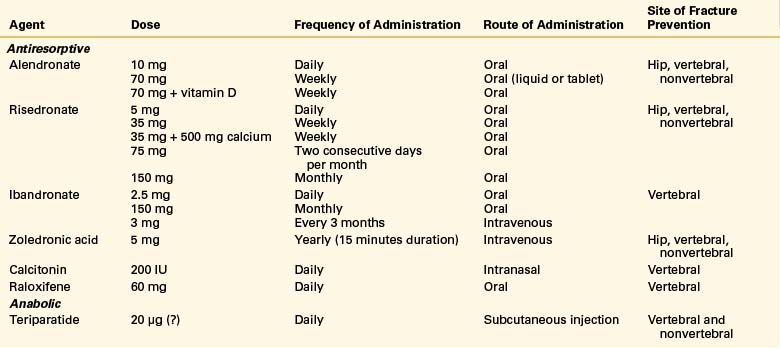
Antiresorptive agents work by inhibiting osteoclast activity, therefore reducing bone resorption. The current available antiresorptives include bisphosphonates, selective estrogen-receptor modulators, and calcitonin.
The bisphosphonates alendronate and risedronate are approved for both the treatment and prevention of osteoporosis. Both alendronate and risedronate have been shown to reduce vertebral and nonvertebral fragility fractures by 50%.47,61–64 Both drugs have also been shown to be effective in the treatment of glucocorticoid-induced osteoporosis.65,66 Another bisphosphonate, ibandronate, which has been approved for the treatment of osteoporosis, has also been shown to reduce the incidence of vertebral fracture by about 50%, but reduction in hip fracture risk remains unproven. An intravenous bisphosphonate, zoledronic acid, has been demonstrated to decrease the incidence of vertebral fractures by 70%, hip fracture by 41%, and nonvertebral fractures by 25% over 3 years in a recent double-blind, placebo-controlled trial of 3889 postmenopausal women with osteoporosis.67 Zoledronic acid is also indicated for the prevention of new clinical fractures in patients who have recently sustained a hip fracture, as it has been shown in a recent study to decrease new clinical fracture and death.68,47
The most common adverse event of bisphosphonates is esophagitis. A higher risk of developing atrial fibrillation with IV zoledronic acid was noted when compared to placebo (1.3% vs. 0.5%); the atrial fibrillation occurred more than 30 days after infusion in most patients.67 The incidence of atrial fibrillation with the treatment of the other bisphosphonates is unclear, and no definitive association has been demonstrated. 47 Rarely, osteonecrosis of the jaw has been reported, mainly in cancer patients receiving high-dose intravenous bisphosphonates. In a recent review article, osteonecrosis of the jaw was rare in osteoporosis patients treated with bisphosphonates, with an estimated incidence of less than 1 case per 100,000; on the basis of the current data, there was insufficient evidence to confirm an association of osteonecrosis of the jaw and low-dose bisphosphonate usage in the treatment of osteoporosis.69 There is currently no consensus on how long to continue bisphosphonate therapy. However, stopping therapy after 5 years for some women may be reasonable, because there appears to be residual benefit on BMD and fractures for 5 years.70
Calcitonin is an antiresorptive hormone for the treatment of osteoporosis in women who are at least 5 years postmenopausal. Calcitonin is administered nasally (200 IU) or subcutaneously. In a 5-year study of postmenopausal women, calcitonin reduced the vertebral fracture risk by 33% to 36% compared to placebo.71 Calcitonin did not decrease the risk of nonvertebral fractures compared to placebo. Unlike other antiresorptives, some patient may experience an analgesic effect from calcitonin that may be of benefit in the treatment of symptomatic vertebral compression fractures.72 This effect may be due to modulation of beta-endorphin levels.73
Raloxifene is an estrogen agonist/antagonist that acts as an estrogen agonist at the bone but an antagonist in uterine and breast tissue in postmenopausal women.47,74 It is approved for both the treatment and prevention of osteoporosis and to reduce the risk of invasive breast cancer in postmenopausal women with osteoporosis.47 Raloxifene has been shown to decrease vertebral fractures by 30% to 50% in postmenopausal women with osteoporosis. It has also been show to increase both spinal and hip BMD.47,75,76 Reduction of hip fracture risk has not been shown. Raloxifene is associated with increased risk of venous thromboembolism and does not decrease the risk of coronary heart disease. Hot flashes are also increased (6% over placebo).47
Teriparatide (recombinant human parathyroid hormone 1-34) is the only currently available anabolic agent that stimulates bone formation by stimulating osteoblasts more than osteoclasts. Administered subcutaneously daily, teriparatide has been shown to increase bone mass by 10% and to decrease vertebral and nonvertebral fracture risk by more than 50%.77 The recommended duration of treatment is a maximum of 2 years, and observational studies suggest benefit for at least 18 months after discontinuation.78 It is common practice to follow teriparatide treatment with an antiresorptive agent, usually a bisphosphonate, to maintain or further increase BMD.79 Several studies have also compared teriparatide with bisphosphonates, and McClung et al. found that 20 μg/day of teriparatide resulted in significantly greater increases in lumbar spine BMD (10.3%) compared to 10 mg/day of alendronate (5.5%).80 Common side effects seen in clinical trials include hypercalcemia, leg cramps, nausea, and dizziness.79 The most serious concern is the risk of osteogenic sarcoma, as rat studies found a dose-dependent increase in teriparatide-treated animals.81 The risk in humans is felt to be small. Patients with an increased risk of osteosarcoma (i.e., Paget disease of the bone); a prior history of radiation therapy of the skeleton, bony metastasis, or hypercalcemia; or a history of a skeletal malignancy should not be treated with teriparatide. This agent should be reserved for patients who are at high risk for fracture or who are unresponsive to or intolerant of antiresorptive drugs.
There is no consensus on the optimal approach for monitoring therapy. The National Osteoporosis Foundation recommends that repeat BMD assessments be performed every 2 years, which is in accordance with Medicare guidelines but recognizes that testing more frequently may be warranted in certain clinical situations.47 Poor compliance and persistence with long-term treatment are major barriers in the management of osteoporosis. Measurement of bone markers has been shown to help overcome such barriers. Suppression of biochemical markers of bone turnover after 3 to 6 months of antiresorptive therapies has been demonstrated.





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


