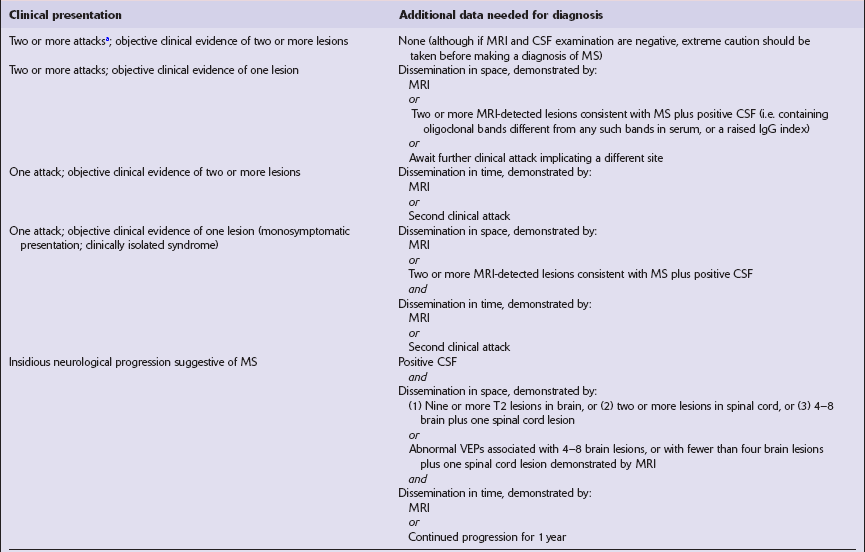
19 Demyelination is characterized by destruction of normal myelin with relative preservation of axons. By convention, the term demyelination excludes disorders in which there is a failure to form myelin normally (dysmyelination) or a loss of myelin as a result of axonal degeneration. The central nervous system (CNS), peripheral nervous system, or both, may be affected by demyelinating diseases. Disorders characterized by a loss of myelin due to an inherited defect of metabolism are considered in Chapter 22. Classical (also known as Charcot-type) MS is classified according to its clinical course as: Until relatively recently, neuromyelitis optica (Dévic’s disease) was classified as a form of multiple sclerosis but in view of its distinct pathogenesis and pathology, it is now regarded as a separate disease (see Chapter 20). Geographic and migration studies • > 30 per 100 000 in most of Europe, Israel, Canada, northern US, southeastern Australia, New Zealand, and easternmost Russia • 5–30 per 100 000 in southern US, most of Australia, South Africa, the southern Mediterranean basin, Russia into Siberia, the Ukraine, and parts of Latin America • <5 per 100 000 in the rest of Asia, Africa, and northern South America. 19.1 Plaques in MS: macroscopic appearance. 19.2 Optic chiasm and nerves in MS. 19.3 Plaques adjacent to the superolateral angle of the lateral ventricles. 19.4 Subpial and junctional plaques. 19.5 Multiple plaques in the deep cerebral gray matter. 19.6 Plaques of demyelination in the brain stem and spinal cord. Several sets of diagnostic criteria have been proposed. Current guidelines are shown in Table 19.1. Table 19.1 aAn episode of neurologic disturbance, of the kind seen in MS, and lasting more than 24 h. Adapted from McDonald WI, Compston A, Edan G, et al. Recommended diagnostic criteria for multiple sclerosis: guidelines from the International Panel on the diagnosis of multiple sclerosis. Ann Neurol 2001; 50:121–127. VEP, visual evoked potential. Plaques containing many lipid-laden macrophages tend to appear slightly yellow or chalky white rather than gray (Fig. 19.7), while old plaques and, rarely, fulminant acute plaques may contain foci of cavitation (Fig. 19.8). 19.7 Plaques of active demyelination in the parieto-occipital region.
Multiple sclerosis
MULTIPLE SCLEROSIS (MS)
CLASSIFICATION
 Relapsing remitting (RRMS), in which the patient experiences multiple acute attacks, each followed by clinical improvement.
Relapsing remitting (RRMS), in which the patient experiences multiple acute attacks, each followed by clinical improvement.
 Commoner in women than men (female:male ratios range from 1.4:1 to 3.1:1 in different studies).
Commoner in women than men (female:male ratios range from 1.4:1 to 3.1:1 in different studies).
 Peak age of onset is 20–40 years; onset before puberty or after 60 years of age is rare.
Peak age of onset is 20–40 years; onset before puberty or after 60 years of age is rare.
 Prevalence varies geographically:
Prevalence varies geographically:
 Low vitamin D level has been implicated as one possible risk factor.
Low vitamin D level has been implicated as one possible risk factor.
CLASSIC (CHARCOT-TYPE) MS
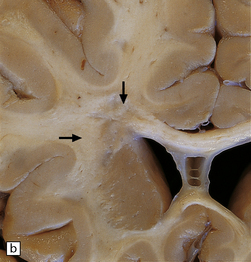
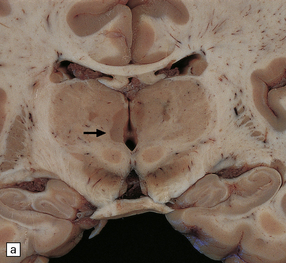
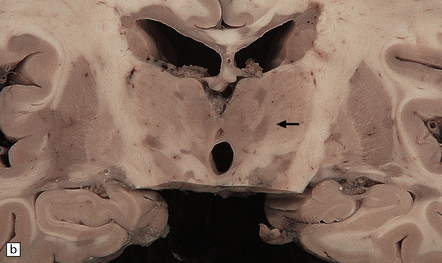
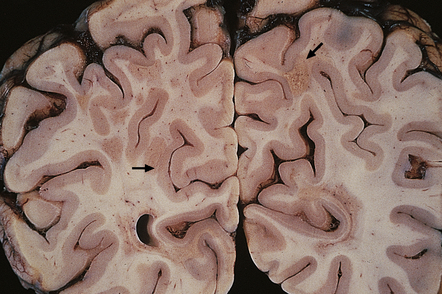
 Vary in size, shape, number, and distribution (Fig. 19.1).
Vary in size, shape, number, and distribution (Fig. 19.1).
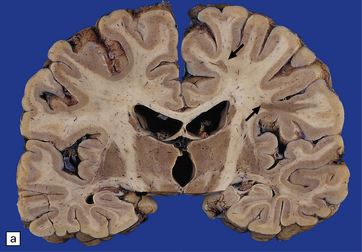
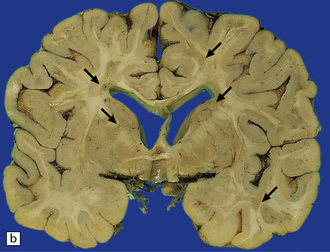


(a,b) Scattered plaques (arrows) of varying shapes, sizes, and locations in coronal brain slices from two patients with MS. (c) Plaques may be visible as slightly depressed areas of gray discoloration on the surface of the pons (arrow), or (d) on the surface of the spinal cord (arrow).
 May extend to the surface of the brain stem and spinal cord, forming gray depressions on external examination (Fig. 19.1).
May extend to the surface of the brain stem and spinal cord, forming gray depressions on external examination (Fig. 19.1).
 May be seen in the olfactory tracts and are frequently present in the optic nerves (Fig. 19.2).
May be seen in the olfactory tracts and are frequently present in the optic nerves (Fig. 19.2).

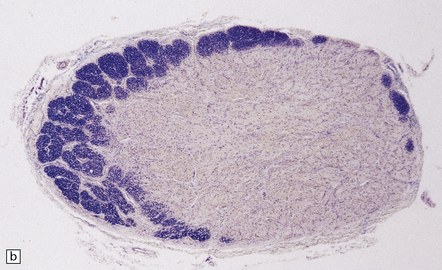
(a) Grayish brown discoloration and atrophy of demyelinated optic chiasm and spinal white matter, most marked in the posterior cervical columns (arrow). (b) Transverse section through optic nerve in which only a peripheral crescent of myelin can still be stained.
 Are often present adjacent to the lateral angles of the lateral ventricles on sectioning the cerebrum (Fig. 19.3).
Are often present adjacent to the lateral angles of the lateral ventricles on sectioning the cerebrum (Fig. 19.3).
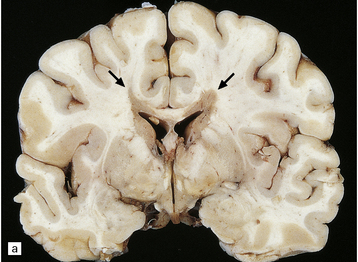
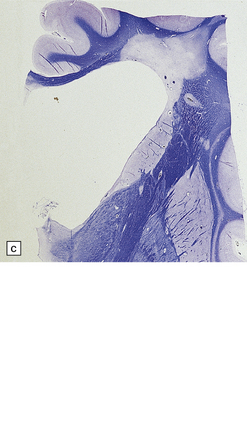
(a,b) In MS, plaques are often found around the superolateral angles of the lateral ventricles (arrows). (c) Staining for myelin reveals a well-circumscribed zone of demyelination (arrows).
 Can occur anywhere in the white matter, at the junction between the cerebral gray and white matter (Fig. 19.4), and within the cortical gray matter and deep gray nuclei (Fig. 19.5), which include myelinated axons as well as neuronal somata and dendrites.
Can occur anywhere in the white matter, at the junction between the cerebral gray and white matter (Fig. 19.4), and within the cortical gray matter and deep gray nuclei (Fig. 19.5), which include myelinated axons as well as neuronal somata and dendrites.
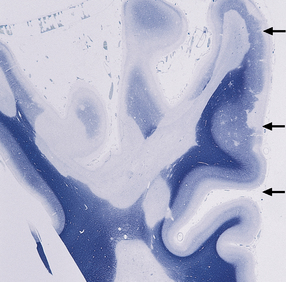
Multiple plaques of demyelination. Here occurring in the subpial region (arrows) and at the junction between cerebral cortex and white matter.
(a,b) These appear as dark gray-brown patches within the basal ganglia and thalamus (arrows to some).
 May occur in the cerebellar white matter and peduncles, in the floor of the fourth ventricle, elsewhere in the brain stem (Fig. 19.6, see also Fig. 19.1c), and in the spinal cord (Fig. 19.6, see also Fig. 19.2a).
May occur in the cerebellar white matter and peduncles, in the floor of the fourth ventricle, elsewhere in the brain stem (Fig. 19.6, see also Fig. 19.1c), and in the spinal cord (Fig. 19.6, see also Fig. 19.2a).
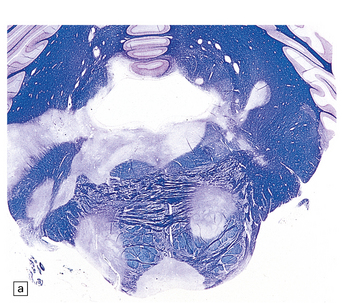
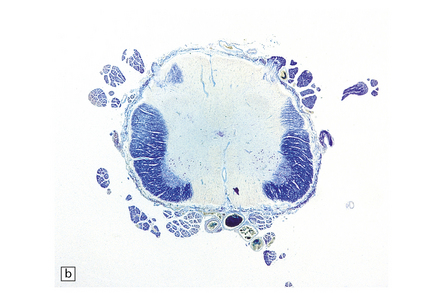
(a) Plaques in the base and tegmentum of the pons. Histology often reveals involvement of the brain stem in MS although the plaques may be difficult to discern on gross examination of the fixed brain. In this case, the weak luxophilic staining in some of the plaques reflects partial remyelination. (b) Extensive demyelination in the lumbar spinal cord. Note the preservation of anterior horn cells.
 Commonly presents with weakness, paresthesia, and sensory loss involving one or more limbs, optic neuritis, diplopia, incoordination, and vertigo.
Commonly presents with weakness, paresthesia, and sensory loss involving one or more limbs, optic neuritis, diplopia, incoordination, and vertigo.
 Often associated with delayed visual evoked responses.
Often associated with delayed visual evoked responses.
Plaques containing large numbers of lipid-laden macrophages tend to have a yellow hue and may have a slightly granular texture (arrows to some).![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Multiple sclerosis






 EPIDEMIOLOGIC ASPECTS OF MS
EPIDEMIOLOGIC ASPECTS OF MS








 IMMUNOLOGIC ASPECTS OF MS
IMMUNOLOGIC ASPECTS OF MS



 MULTIPLE SCLEROSIS
MULTIPLE SCLEROSIS





Only gold members can continue reading. Log In or Register to continue

