Myoclonic Absences: The Seizure and The Syndrome
Michelle Bureau*
Carlo Alberto Tassinari†
*Centre Saint-Paul, Hôpital Henri Gastaut, Marseille, France
†Ospedale Bellaria, Bologna, Italy
Introduction
Myoclonic absences (MA) represent a specific seizure type, whose diagnosis rests on clinical observation and ictal polygraphic and EEG-video recording. Clinically MA are characterized by rhythmic and bilateral jerks of the limbs. The ictal electroencephalogram shows a rhythmic, bilateral, synchronous, and symmetric spike-and-wave discharge at 3 Hz associated with myoclonias rhythmically repeated at 3 Hz and an increasing tonic contraction.
Since the first description by Tassinari et al. in 1969, 1971 (1,2), and later in 1985 (3), the authors stressed the fact that MA represent an individual seizure type and proposed the existence of a specific epileptic syndrome in which MA were the only or the predominant seizure type. It should thus be separated from other forms of generalized epilepsy, such as childhood absence epilepsy (CAE). Indeed, MA were shown to be most often associated with mental retardation and a resistance to medical treatment so that the prognosis was more severe than in idiopathic generalized epilepsy (IGE).
The 1989 International classification of epilepsies and epileptic syndromes eventually recognized that epilepsy with MA was a separate entity and included it in the group of cryptogenic or symptomatic generalized epilepsies (4). This can be found in the new proposed diagnostic scheme for people with epileptic seizures and with epilepsy (5). Epilepsy with MA is maintained in epilepsy syndromes and related conditions.
The Myoclonic Absence: A Specific Seizure Type
Clinical Symptomatology
Motor Manifestations
The myoclonias constitute the constant characteristic feature, often associated with more or less tonic contraction. The myoclonias mainly involve the muscles of the shoulders, arms, and legs. The muscles of the face are less frequently involved. When this occurs, they are more evident around the chin and the mouth, whereas twitching eyelids is typically absent or rare.
Due to concomitant tonic contraction, the jerking of the arms is accompanied by a progressive elevation of the upper extremities, giving rise to a quite constant and recognizable pattern. When the patient is standing, falling is uncommon but a backward or forward oscillation is frequently seen. Head and body deviation (without concomitant ocular or oculoclonic deviation) can be observed in some cases. In some cases slight automatic movements were observed.
Impairment of consciousness is of variable intensity, ranging from a complete loss of consciousness to a mild disruption of contact. Sometimes the myoclonias are felt as a very disturbing experience; the subject frequently holds himself, giving the impression of attempting to control the intensity of the jerking. He may recall the words pronounced by the examiner during the seizure.
Autonomic Manifestations
In some cases a change or an arrest of respiration and sometimes a loss of urine can be noted.
The MA have an abrupt onset and termination
The duration ranges from 10 to 60 s (longer than usually observed in CAE)
The frequency is high and MA occur at least several times per day–often tens of times per day. They are often provoked by hyperventilation or awakening. In 14% of cases, they can be elicited by intermittent photic stimulation (ILS). MA can occur during light sleep, sometimes awakening the patient. Episodes of MA status are distinctly rare [1 case among 36 cases reported by Tassinari et al. (6)].
EEG and Polygraphic Symptomatology
The ictal EEG consists of rhythmic spike-and-wave discharge at 3 Hz, bilateral, synchronous, and symmetric, as observed in the absences of CAE. The onset and the end of the spike-waves are abrupt, except in rare cases in which the EEG discharge ends progressively, sometimes with asymmetric delta waves over the frontal areas. In some seizures, typical spike-waves can be intermixed with polyspikes
The polygraphic recording discloses the appearance of bilateral and rhythmic myoclonias, at the same frequency as the spike-waves, beginning about 1 s after the onset of the EEG discharge. Later into the seizure, the myoclonias are associated with a tonic contraction that is maximal on the shoulder and deltoid muscles and that is responsible for the elevation of the arms (Fig. 13-1). The tonic contraction can mask or render the myoclonias clinically less evident; the motor manifestations are thus less evident. Sometimes the myoclonias and the tonic contraction are unilateral or clearly asymmetric (Fig. 13-2) (with a jerky rotation of head and trunk) despite the generalized EEG pattern (Fig. 13-3).
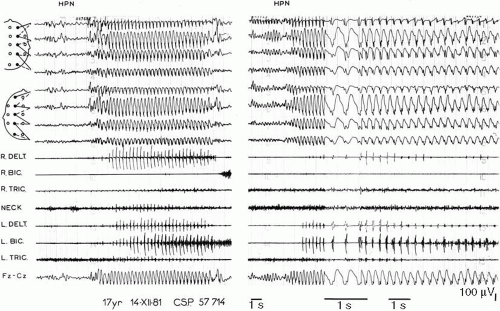 FIG. 13-1. Myoclonic absences (MA) elicited by hyperventilation. Left: MA characterized by a 3-Hz spike-and-waves discharge. Note that the rhythmic jerks (recorded on the right and left deltoids, biceps and triceps muscles, and on the neck) appear 1 to 2 s after the onset of the spike-wave discharge and that the tonic contraction appears 3 to 4 s later, mainly on the left deltoid. Right: another MA, recorded at 30 mm/s. |
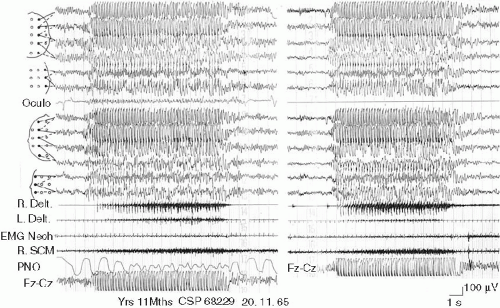 FIG. 13-2. Myoclonic absences in a 6 year 11 month old boy. Note the asymmetry of the myoclonias and the tonic contraction that is more intense on the right deltoid than on the left. |
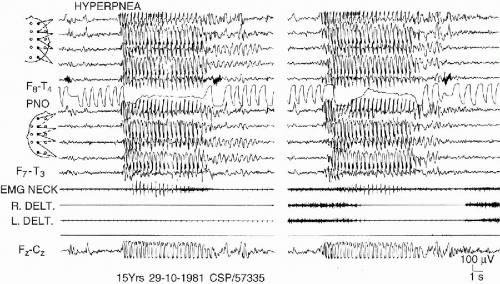 FIG. 13-3. MA elicited by hyperventilation. The myoclonic jerks involve only the neck muscles causing a jerky rotation of head. |
Tassinari et al. (1,2) proved, by means of high-speed oscilloscopic recording, that there is a strict and constant relation between the spike-wave discharge and the myoclonias. The detailed morphology of spikes shows a positive transient (7) of high amplitude in strict relationship with the appearance, latency, and amplitude of the myoclonias. Each spike on the EEG is followed on the electromyography (EMG) by a myoclonia with a latency of 15 to 40 msec for the more proximal muscles and of 50 to 70 msec for the more distal muscles. This myoclonia is again followed by a brief silent period (60 to 120 msec) that interrupts the tonic contraction.
At times, the spike-wave in the first second are of smaller amplitude (because the early positive component of the spike is of small amplitude) and are not accompanied by myoclonias (Fig. 13-4).
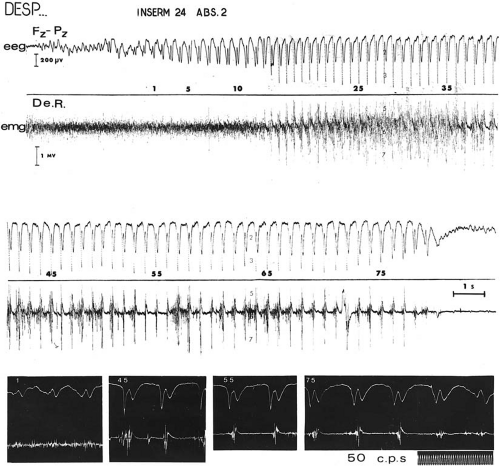 FIG. 13-4. Polygraphic recording of a myoclonic absence with only 1 EEG lead (Fz-Pz). Note that low-amplitude spike-wave precedes the onset of myoclonic jerks and of tonic contraction, which are correlated with an increase of amplitude of the spike-wave. The myoclonias last as long as the spike-wave discharge, while the tonic contraction resolves during the absence. |
The awake interictal EEG shows a normal background activity for age in all cases. We have never recorded the sinusoidal slow rhythm in the posterior areas, as has been observed in CAE. Generalized spike-waves are noted in one-third of cases and, more rarely, focal or multifocal anomalies. ILS is without effect except when it elicits MA.
Myoclonic Absences and Sleep
Sleep organization is constantly normal and physiologic patterns (vertex spikes, K complexes, spindles) are present bilaterally and symmetrically. The evolution of interictal spike-wave discharges during sleep is similar to that observed in CAE (8). The MA can occur during stage I of sleep, sometimes awakening the patient (Fig. 13-5). Generalized spike-wave discharges of variable duration (25–10 s), that are sometimes associated with bursts of myoclonias, can be observed during sleep stages II and III. Isolated spikes or irregular spike-waves predominating on one or the other anterior regions are frequent during slow sleep. On the other hand, no other interictal discharges are recorded and, particularly, no bursts of fast rhythms at 10 Hz as observed in the Lennox-Gastaut syndrome (LGS).
Related posts:
 Progressive Myoclonus Epilepsies: EPM1, EPM2A, EPM2B
Progressive Myoclonus Epilepsies: EPM1, EPM2A, EPM2B
 Myoclonic Status in Nonprogressive Encephalopathies
Myoclonic Status in Nonprogressive Encephalopathies
 Myoclonic–Astatic Epilepsy of Early Childhood – Definition, Course, Nosography, and Genetics
Myoclonic–Astatic Epilepsy of Early Childhood – Definition, Course, Nosography, and Genetics
 Familial Juvenile Myoclonic Epilepsy
Ketogenic Diet in Patients with Dravet Syndrome and Myoclonic Epilepsies in Infancy and Early Childhood
Familial Juvenile Myoclonic Epilepsy
Ketogenic Diet in Patients with Dravet Syndrome and Myoclonic Epilepsies in Infancy and Early Childhood
 Treatment of Myoclonic Epilepsies of Childhood, Adolescence, and Adulthood
Treatment of Myoclonic Epilepsies of Childhood, Adolescence, and Adulthood
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


