(1)
Department of Neurosurgery, St Elisabeth-Tweesteden Hospital, Tilburg, The Netherlands
After World War II, the centre of gravity in aphasiology research shifted from Europe to North America [1]. In this period, interest in the German and French localist theories waned to virtual non-existence in clinical practice. The localist view was replaced by ideas with a more holistic character. A factor that likely contributed to this transition was the many war casualties, whose complex disturbances and potential for recovery were not very well explained by the contemporary language theories. These observations triggered basic research on aphasia, as well as efforts to rehabilitate patients [2]. Somehow, then, interest renewed to a point where localism again became the dominant clinical view that it remains today.
7.1 Geschwind
One of the investigators who contributed much to this renaissance was Norman Geschwind (1926–1984), who summarized his own view on historical findings as follows (1974):
It is worth recalling what the state of the art was in 1961. Until the First World War the accomplishments in the field of understanding the relationships of the brain to language had been rightly regarded as among the brightest treasures of the discipline of clinical neurology, and the list of major contributers to it would have included a majority of the creators of the discipline—Broca, Meynert, Flechsig, Jackson, Wernicke, Liepmann, Lichtheim, Dejerine, to mention only a few.
Yet by the 1950s interest in the area had nearly vanished from the field of clinical neurology. There were a few exceptions, such as Luria in the Soviet Union, but much of his work has been published only recently. In all of the French, German, and English-speaking worlds there were probably not a dozen neurologists for whom the higher functions of the brain represented a major interest [3].
Geschwind’s training as a neurologist imbued him with ‘an overwhelming skepticism toward the view that there were highly characteristic aphasic syndromes associated with different lesions of the brain’ [3]. The dominant theories of that time were strongly holistic. As he himself explained, he had ‘forcefully (…) accepted the view that any attempt at “explaining” the syndromes on the basis of anatomy was a futile endeavor’ [3]. At that time Geschwind also regarded himself a believer of the ideas of more holistic-orientated neurologists such as Jackson, Goldstein and Head. Triggered by some of his teachers and the recent work of Myers and Sperry on callosum-sectioned animals, he began doubting these ideas and decided to study the classic localizationist school by reading the original papers ‘rather than by reading the interpretations of later hostile authors’ [3–4]. As he recalls in his Selected Papers on Language and the Brain (1979):
Somewhere about 1960 I awoke, perhaps belatedly, to my own profound confusion. (…) I was persistently troubled by the fact that people who had left their mark so indelibly in many areas of neurology, such as Wernicke, Bastian, Dejerine, Charcot, and many others, could apparently have shown what was asserted to be the sheerest naiveté and incompetence in the area of higher functions. It seemed difficult to accept the view that men who had established long-honored clinical pictures should have apparently been so incapable of examining an aphasic, or that scholars who had made fundamental anatomical investigations of permanent worth should have been so perfunctory and sloppy in their descriptions of the brains of aphasics [3].
The first paper he read was that of Dejerine on his case of pure alexia without agraphia (the case was briefly described in Fig. 4.5 in Chap. 4):
The impact of the paper was multiple. In the first place the description was so lucid that it was immediately clear that this ‘pure’ syndrome must exist, despite the insistence of some modern writers that these selective syndromes ‘could no longer be seen’ (a statement implying that the earlier descriptions had been grossly in error). Indeed it was obvious that Dejerine’s standard of examination was superior to that of most modern students of aphasia. Furthermore it was a shock, but a salutary one, to discover that even so masterful a paper had been neglected by later writers, or grossly misquoted. Henry Head (1926), the often cited critic of classical approaches, did not even list it in his biography. This paper was therefore instrumental in making me aware of the inaccuracy of most of the histories of aphasia in English. [3]
Within a few weeks after reading this paper, Geschwind observed a similar case himself. Not much later he came across another callosal case. This patient had initially been seen by a colleague, Edith Kaplan. The patient had undergone surgery for a left frontal glioblastoma. After surgery, Kaplan found out that the man could write normally with his right hand, but—astonishingly—wrote aphasically with his left hand. In a book that is a tribute to Geschwind, Devinsky (1997) writes about this case:
She [Kaplan] could have told a thousand neurologists about this case, and it would have remained one of those curiosities that doesn’t seem to fit into the comfortable pigeon-holes of knowledge, but she told Norman Geschwind. (…) The timing was fortuitous, but Pasteur’s dictum applied – chance favors the prepared mind [5].
The 41-year-old patient presented with headache, nausea and vomiting. Members of the family had noticed increasing behavioural changes over the previous months. The patient was right-handed and, except for a few paraphasias and some hesitancy in naming objects, had normal speech. Further neurological examination revealed an alert and cooperative patient with considerable frontal lobe dysfunction:
He exhibited inappropriate jocularity against a background of general apathy. He had no insight into his illness and appeared unconcerned about it. He kept repeating questions as if he did not quite understand them. He could remember only 1 of 3 items after five minutes. He repeated 6 digits forward and 4 backward. He made many errors in subtracting sevens serially from 100. His proverb interpretations were very poor, being little more than restatements without interpretation. He did simple written arithmetic correctly but failed on more complex material such as multiplying 214 by 35. When asked to draw a clock face at a certain hour, he frequently reversed the large and small hands [5].
After surgery (where a partial left frontal lobectomy had been performed), there was initially a dense right hemiplegia and a marked aphasia. This partially improved with time, in particular the language abilities. One and half months after surgery, the patient’s speech showed ‘at most a few paraphasic errors’, although he ‘followed complex commands poorly’. Neuropsychological examination showed no essential differences as compared with the preoperative test results. Around that time it was discovered that the patient had writing difficulties with his left (!) hand. Upon subsequent testing, several other unusual findings were found, based on an aphasic disturbance in naming:
He named objects placed in the left hand (concealed from vision) incorrectly; he could select them afterwards with his left hand by touch or pointing; and he could draw the object afterwards with his left hand. Even while giving an incorrect verbal description, he could demonstrate correctly the use of the object being held in the left hand. If an object was placed in one hand (concealed from vision), he could not select it from a group or draw it with the other hand. He frequently performed verbal commands incorrectly with his left hand.
The authors feel that the simplest explanation of the phenomena is that the patient behaved as if his two cerebral hemispheres were disconnected and that the probable cause of this was a lesion in the corpus callosum [5].
Kaplan and Geschwind reasoned that as a consequence of surgery, the anterior portion of the corpus callosum had been lesioned, thereby disconnecting left hemisphere language areas from the right hemisphere areas that controlled the left hand (this was later confirmed in post-mortem examination) [6]. They presented this case of tactile aphasia, as well as the one with alexia without agraphia, at a conference in 1961. A brief report of this meeting was published in The New England Journal of Medicine [7] and a full paper somewhat later in Neurology [8]. From that period on, Geschwind and collaborators further elaborated on the behavioural syndromes that resulted from localized brain lesions and in particular on the various ‘syndromes of disconnection’. Geschwind is not only to be credited for these efforts, and as a founder and teacher of the new discipline of behavioural neurology, but also for ‘resurrecting the German and French literature from the late nineteenth and early twentieth centuries that had been buried by neglect and misinterpretation’ [5]. It is indeed striking to read in his work the many references to the historical literature and his tributes to its many pioneering authors. A genuine surprise can often be felt with him when he describes in his papers that many of his cases and syndromes that he initially thought were original and new had been so eloquently documented in the past:
What was astonishing [Geschwind is now referring to the works of Dejerine and Liepmann on callosal disorders] was the fact that this work had been so grossly neglected. It was published in widely-read journals and received wide acclaim in its day. Indeed, it was discussed fully in Lange’s (1936) article contained in the standard German neurological reference, the Bumke-Foerster Handbuch. Furthermore, Liepmann’s results had been reported with Otto Maas, who was still alive in the 1950s and had been confirmed by a whole array of authors such as Kurt Goldstein, who himself described a callosal syndrome in 1908. Despite this fact, the students of Kurt Goldstein whom I met were generally unaware of this fact.
I was again made aware not merely of how inaccurate most of the histories of the higher functions were, but also that important confirmed scientific observations could almost be expunged from the knowledge of contemporary scientists. My presumption is that this must occur in other fields as well. The reasons for this phenomenon were fairly standard: neglect of work written in a foreign language, neglect of work done by someone in a different field, excessive reliance on the authority of certain towering individual figures. [3]
Geschwind wrote several papers that directly aimed to correct some of the ‘grossly incorrect views’ on historical events and some of its key figures. For instance, in a lengthy paper, he pays tribute to Meynert and Wernicke, re-analysing their work and restating the importance of their contributions for modern neurology and neuroscience [9]. Geschwind was also keen to acknowledge some errors in Wernicke’s earliest work, in particular regarding the concept of his conjunction aphasia [Leitungsaphasie]:
There was, however, an even more important source of error which resulted from Wernicke having failed to analyze his own diagram correctly; he had omitted the deduction that there should be a disturbance of repetition in conduction aphasia. Lichtheim in 1885 correctly added the deduction and cited a patient showing this condition [10]. Freud returned to this problem in 1891 and, although he cited Lichtheim extensively, he seemed to have missed in part some of Lichtheim’s extension of Wernicke’s theory [11]. Freud argued, as Lichtheim had, that the lesion disconnecting the motor from the sensory speech area should produce a loss of repetition in the face of intact comprehension, and went on to remark that this situation is highly unlikely. Yet within the next twenty years the triad of paraphasia, intact comprehension and impaired repetition was to become well known. In 1904 Karl Kleist, then an assistant of Wernicke’s at Halle, demonstrated a case which convinced Wernicke of the existence of this entity. [3]
Geschwind refined and expanded the older connectionist view into what some have called neo-associationism [12]. In 1961, Geschwind met Zangwill, who was at the time an associate editor of the journal Brain. Zangwill persuaded him to expand his ideas on callosal disconnections, and this led to Geschwind’s landmark paper, ‘Disconnexion syndromes in animal and man’, which was published in Brain in 1965. This paper, which was essentially a monograph, spanned 116 unillustrated pages and was published in two parts for editorial reasons [13, 14]. The work starts with anatomical considerations on connecting pathways in the brain and in particular with Geschwind’s description and ‘rediscovery’ of Flechsig’s rule (1901). This rule states that ‘primary receptive areas (…) have no direct neocortical connexions except with immediate adjacent, “parasensory” areas’ [13, 15]. Thus, according to Flechsig, all cortical connections between primary sensory areas pass through surrounding areas of associative cortex, and there are no direct intra-hemispheric connections between these areas (there are—of course—direct connections to and from subcortical areas, e.g. via the thalamus). Geschwind generalized the rule to include also primary motor cortex and inter-hemispheric connections [12, 13].
Flechsig (1847–1929) was a German neuroanatomist who is remembered best for his work on myelination of the central nervous system. He had noted that different areas myelinated at different times during embryonic and postnatal development of the brain and ‘introduced the ‘fundamental law of myelinogenesis’ that the sequence of myelination during individual development repeats their phylogenetic appearance’ [16]. Flechsig categorized cerebral areas into three large groups, depending on their state of myelination. The ‘primordial regions’ were those areas that were already myelinated before birth; these areas largely correspond to the ‘primary sensorimotor areas’ (see also Fig. 7.1). The second group consisted of ‘intermediate areas’ that were myelinated approximately 1 month after birth. Finally, there were ‘terminal areas’ that myelinated even later than that. Flechsig was led by the idea that evolutionarily younger systems myelinated later than the phylogenetically older and more primitive systems. He linked this temporal differentiation in myelination to differences in brain functions. The slower the development of an area, the more ‘higher’ intellectual brain functions were performed by that area. Flechsig named these areas ‘associative centres’:

Fig. 7.1
Flechsig’s myelogenetic map of the human cortex (1901). Flechsig constructed a brain map that initially consisted of 40 areas; later he reduced the total to 36. The coloured areas constitute the so-called primordial zones that are already myelinated at birth. Myelinization of the other areas is completed in later stages. Numbers reflect the chronological order of myelinization (Figure taken from Catani and ffytche, 2005 [12])
Flechsig (1905) thought his posterior association center [located in the temporoparietal region] was the most important part of the brain for intellectual functions. He wrote that the posterior association center was responsible for connecting words with their content, understanding notations, forming intellectual conceptions of the external world, and grasping complex situations. In contrast, Flechsig emphasized the role of the frontal cortex in emotion and consciousness, but concluded that the frontal lobes were not the centers for abstract thinking, as Eduard Hitzig had proposed. [17]
For Geschwind, Flechsig’s rule and his forgotten work was an important part of his theories, whereby lesions to association cortex itself could lead to disconnection syndromes:
These anatomical facts imply that a large lesion of the association areas around a primary sensory area will act to disconnect it from other parts of the neocortex. Thus, a ‘disconnexion lesion’ will be a large lesion either of association cortex or of the white matter leading from this association cortex. The specification of the association areas as way-stations between different parts of the neocortex is certainly too narrow, but it is at least not incorrect. This view, as we shall see, simplifies considerably the analysis of effects of lesions of these regions. Since a primary sensory region has no callosal connections, a lesion of association cortex may serve both to disconnect such an area from other regions in the same hemisphere and also to act in effect as a lesion of the callosal pathway from this primary sensory area. [13]
Geschwind’s theories were also shaped by other evolutionary facts (see also Catani’s excellent review The rises and falls of disconnection syndromes [12]). In subprimate animals, Flechsig’s rule does not hold, and the primary sensory cortices of different modalities are connected either directly or via the limbic system [12]. As organisms ascend the evolutionary ladder, associative areas arise and these ‘associative areas become separated to a great extent from the receptive’. Primary sensory areas become surrounded by associative cortical regions. In the monkey, associative cortices are connected to one another via the limbic system, and all primary cortices are thus indirectly connected via associative cortex and the limbic system. In man, according to Geschwind, a higher-order associative area developed in the inferior parietal lobe, and this area was able to integrate information from multiple modalities independent of the limbic system. It formed at the crossroads of visual, auditory and sensory areas. Geschwind calls this area the ‘association area of association areas’ (i.e. a secondary association area). He speculated that this area freed humans from the dominant pattern of sensory-limbic associations, and postulated that the evolutionary development of language was dependent on the emergence of this parietal association area (1965):
The situation (…) is not simply a slightly more complex version of the situation in the higher primates but depends on the introduction of a new anatomical structure, the human inferior parietal lobule, which includes the angular and supra marginal gyri, to a rough approximation areas 39 and 40 of Brodmann. In keeping with the views of many anatomists Crosby et al. (1962) comment that these areas have not been recognized in the macaque. Critchley (1953), in his review of the anatomy of this region, says that even in the higher apes these areas are present only in rudimentary form. (…) In addition this area is one of the late myelinating regions or ‘terminal zones’ as Flechsig termed them. In fact, this region was, in Flechsig’s map, one of the last three to myelinate. (…) Yakovlev (personal communication) has pointed out that this region matures cytoarchitectonically very late, often in late childhood. [13]
7.1.1 Neo-connectionism
Geschwind’s language model was essentially a modification of that of Wernicke and Lichtheim; hence, it is now usually referred to as the Wernicke–(Lichtheim–)Geschwind model of language [18, 19]. Geschwind built on the traditional approach whereby words are transferred from one region to another, the regions being interconnected as functionally distinct modules. It is of note that the only connection that is anatomically specified is the arcuate fasciculus, although even of this pathway, the exact course and terminations are not given. Geschwind agreed with Wernicke—and later Konorski (1961), who revived interest in conduction aphasia—that conduction aphasia was best explained by a lesion of the arcuate fasciculus [13]. Geschwind added the angular region as a centre for ‘visual word memory’—or ‘more correctly’—the region of the temporoparietal-occipital junction. Within this region, written language is turned into spoken language and vice versa. It contains the ‘rules for associating stimuli in two modalities, i.e. visual and auditory’ [3]:
Thus a visual stimulation can evoke an auditory association by means of the pathway: visual cortex—visual association cortex—angular gyrus—auditory association cortex. The auditory association cortex shown here [Fig. 7.2, top left] is the classical Wernicke’s area. Broca’s region is a region of motor association cortex lying anterior to the face region of the classical motor cortex. It may be thought of as containing the learned rules for translating a particular heard sound pattern into a motor sequence. [3]

Fig. 7.2
Some of the schemes that Geschwind (1969) used to illustrate his ideas of the organization of auditory and visual language functions in the brain [3]. (Left) (1) face area of motor cortex, (2) Broca’s area, (3) lesion involving arcuate fasciculus (dotted lines), (4) Wernicke’s area and (5) angular gyrus. (Figure taken from Geschwind, 1974 [3]). (Right) ‘Linguistic competence requires the cooperation of several areas of the cortex. When a word is heard (upper diagram), the sensation from the ears is received by the primary auditory cortex, but the word cannot be understood until the signal has been processed in Wernicke’s area nearby. If the word is to be spoken, some representations of it is thought to be transmitted from Wernicke’s to Broca’s area, through a bundle of nerve fibers called the arcuate fasciculus. In Broca’s area the word evokes a detailed program of articulation, which is supplied to the face area of the motor cortex. The motor cortex in turn drives the muscles of the lips, the tongue, the larynx and so on. When a written word is read (lower diagram), the sensation is first registered by the primary visual cortex. It is then thought to be relayed to the angular gyrus, which associates the visual form of the word with the corresponding auditory patterns in Wernicke’s area. Speaking the word then draws on the same systems of neurons as before’ (Figure and text taken from Geschwind, 1979 [128])
The model permits certain new predictions, for instance, that lesions in Wernicke’s area will also lead to problems with written language, as seen words cannot longer arouse their auditory forms. However, this was, and still is, a matter of debate:
Some of the classical authors were inclined to feel that the sight of an object could directly arouse the written production. (…) But what makes this supposition unlikely is that writing is invariably abnormal in patients with the speech pattern of Wernicke’s aphasia, while one might expect it to be spared at least occasionally if this were the case. Hence it appears that to write the word, the spoken form must be aroused first. [3]
Geschwind realized that his model had limitations and that not all aphasic phenomena could be adequately explained by it. This is extensively discussed in his work, and—when appropriate—possible solutions are suggested. For instance, in case of writing disturbances, Geschwind hypothesized a separate pathway from the angular gyrus to Broca’s area that ‘runs forward and mixes in the lower parietal lobe with the fibers from Wernicke’s area’ [3]. Despite the shortcomings, Geschwind considered the anatomical approach the best way to explain the known data, as well as a good starting point for experimental testing of new hypotheses. Of course, Geschwind knew that reality was far more complex than his reductionist model, a fact he kept repeating in his work:
By far the most common types of criticism of the lesion method have been based on (a) the inappropriate attribution of a lost function to the locus of a lesion, and (b) exceptions to and inconsistencies of anatomical localization. Only an uninformed or naive thinker can believe that Wernicke regarded the area which came to carry his name as the site where the full process of auditory comprehension took place; yet, Wernicke and many of his most important followers have been accused of precisely that belief. No effort should be spared to make it clear that the effects of a circumscribed locus of damage can be understood only by taking into account that the healthy brain tissue that has been destroyed was a component of a neural network, the activity of which mediates the normal function; and furthermore, that to understand post-lesional alterations in function one must take into account changes in other parts of that network.
The argument regarding exceptions and inconsistencies in localization depends, as usually stated, on invalid assumptions. No one can disagree with the assertion that exceptions or inconsistencies demand attention. In some instances they lead to the realization that the asserted localization is incorrect, and thus serve the same function that discrepant data serve in every branch of science. All to often, however, the argument is advanced that the existence of discrepancies shows that the very concept of localization of function is untenable. Implicit in this argument is the belief that a particular localization is acceptable only if it is universally valid. (…) It is clear that, in order to establish a valid correlation between disordered behavior and the site of anatomical brain damage related to it, it is necessary to take into account a large number of factors, the principal of which are: (a) the nature of the pathological process, (b) the size of the lesion, (c) the speed of the pathological process, (d) the timing of anatomical and behavioral observations, (e) individual variations in neurological organization, (f) the age, level of education, sex, and premorbid psychological and social factors of the individual under study. [20]
Geschwind and Wernicke shared a common opinion on many issues. Geschwind regarded the loss of Wernicke’s area as the destruction of a memory store, ‘as it was in fact regarded classically’ [13]. He named Wernicke’s area ‘the storehouse of auditory associations’ [13]. When a name passes through Wernicke’s area and the angular gyrus, it will arouse associations in the other parts of the brain. ‘It is probably thus that Wernicke’s area attains its essential importance in “comprehension”, i.e. the arousal of associations’. Geschwind and Wernicke also shared a similar critical view on agnosia and its interrelationship with aphasic disturbances, stressing that these are not two distinct physiological phenomena (see also Chap. 3). Geschwind held the opinion that the contemporary criteria that had been formulated to classify abnormal behaviour into one or the other category were inadequate:
The fundamental difficulty has been in the acceptance of a special class of deficits of ‘recognition’, lying somewhere between defects of ‘perception’ and ‘naming’. What indeed are the criteria for ‘recognition’ and is it a single function? I believe in fact that there is no single faculty of ‘recognition’ but that the term covers the totality of all the associations aroused by any object. (…) this view abolishes the notion of a unitary step of ‘recognition’; instead, there are multiple parallel processes of appropriate response to a stimulus. [14]
Geschwind’s neoclassical approach in the 1960s became internationally known, and Wernicke’s classification was to some extent ‘repackaged as the Boston classification’ [1]. The Boston School became renowned for its research on aphasia and for a test battery that was developed by Goodglass and Kaplan, the Boston Diagnostic Aphasia Examination [21]. This battery, developed at a time when brain imaging was still in its infancy, aimed to localize structural lesion from impaired functions [1]. Until today, Geschwind’s legacy remains a prominent part of our clinical approach to patients with aphasia.
7.2 Luria
Alexandr Romanovitsj Luria (1902–1977) was a Soviet psychologist whose work had a great influence on (Western) modern neuropsychology and cognitive neuroscience. He was one of the leading psychologists of the twentieth century and is considered one of the founders of modern neuropsychology and cognitive neuroscience. His work covered many different topics and has been characterized by adjectives such as dynamic, functional and evolutionary [22].
Luria graduated from university in 1921, aged just 19. While still a student, he established the Kazan Psychoanalytic Association and planned a career as a psychologist [23]. Initially, he worked on methods that could objectively measure abnormal mental processes, based on theories of Jung and Freud. At the time, Luria’s intellectual life was heavily influenced by German writings. German was the family’s second language, and Luria had learned it at an early age. He was therefore able to read German literature long before it would be available in Russian translation [23].
In 1924, Luria met Lev Vygotsky (1896–1934), who would become his lifelong teacher and friend. In Vygotsky’s view, higher mental processes are predominantly the result of a person’s complex social–historical development. ‘They are formed under the influence of people’s concrete activity in the process of their communication with each other and in fact always represent complex functional systems based on jointly working zones in the brain’ [24]. Luria based his work on this more philosophical approach of Vygotsky, attributing a large role to a person’s environment as a determinant of his or her individual behaviour. He thereby maintained a more comprehensive view than would have been possible if he had endorsed either the psychic or physical reductionist positions [25]. Later in life, Luria also embarked on a career in neurology and was able to link theories of higher mental functions and language to anatomical and clinical evidence of brain dysfunction. Throughout his whole career, he tried to fuse elements of the biological and the environmental approach, as for him the study of the individual brain alone was not sufficient to reveal the organization of complex behaviour [26]. In addition to that, Luria stated in his autobiography:
The time was long past to consider psychological processes as the results of either strictly localized brain activities or the ‘mass action’ of the brain in which all of its parts were ‘equipotential’. It was time for us to begin the next step in our work: to explain the neurophysiological or, to use a Russian phrase, ‘neurodynamic’ mechanisms underlying the activity of brain loci implicated in specific syndromes. (…) Progress depended upon advances in both of the areas that had concerned me all my life. On the one hand, I had to move from brain structures to a deeper understanding of the neurophysiological mechanisms that were operating in these structures. On the other hand, our psychological analysis of higher cortical functions was by no means complete, and we needed improved psychological analyses as well. To signify the combination of these two enterprises, the ‘neurological’ and the ‘psychological’, the term neuropsychology was coined. Developing this field of science has taken a long time and the help of many people [26].
For a large part of his professional life, Luria worked in Moscow’s Burdenko Institute of Neurosurgery. Intracranial cases from all over Russia were referred to this large (300-bed) institute. After the outbreak of World War II, it became in fact an enormous testing ground for new neuropsychological approaches, as Luria organized a rehabilitation hospital for the massive numbers of brain-injured patients. This was fertile ground to develop new techniques to diagnose and localize brain lesions and to restore lost neurological functions (Fig. 7.3) [26]. Besides the huge number of cases available, it was of great advantage that the location of the lesion was often known because of surgical findings or post-mortem examinations. One of Luria’s many books, Traumatic Aphasia: Its Syndromes, Psychology and Treatment, resulted from these experiences and was published in 1947 [27]. Unfortunately, it did not appear in English translation until as late as 1970 [28]. Geschwind, in a review of this book, acknowledged its great importance and called Luria ‘one of the modern giants in the field’:
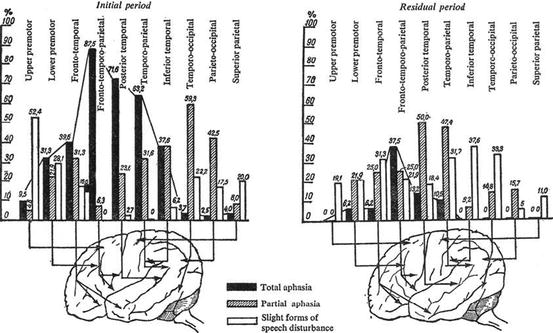
Fig. 7.3
Luria (1947) systematically documented traumatic aphasia in war casualties [27]. The diagrams show the distribution of speech disturbances from gunshot wounds to different parts of the brain in approximately 800 patients. The vertical axis indicates the percentage of speech disorders (of various degrees of severity) as a function of the particular area of the left hemisphere that was damaged. Note that Luria studied patients for some time after the initial brain injury in order to capture the effects of recovery (Figure and text (adapted) from Luria (1970) [28])
Indeed, some of Luria’s original contributions, as expressed in his other writings over the past twenty years, have become such integral components of thought in this area, and have appeared so frequently in the writings of others—who often fail to realize their origin—that we are likely to underestimate the statue of this book. At the time of its publication in 1947, it was undoubtedly the most important work on aphasia since the close of the classical period in the 1920s. Had it been translated into English at the time, it might have hastened the modern revival of interest in this area in France, Germany and the English-speaking countries, where knowledge of Russian and even sensitivity to the possibility of important Soviet contributions were unfortunately generally lacking [22].
7.2.1 Functional Systems
Luria regarded ‘functions’ as complex functional systems with dynamic levels of localization in the brain. He defined a function as a complex form of goal-directed adaptive behaviour and characterized functions by the variability of the participating systems. Take for instance locomotion, which can be achieved by different sets of muscles; or writing, which can be achieved both by mouth or foot if required by circumstances [29]. Initial ideas on functional systems in Russia had been formulated by Anokhin [30] and Bernstein [31] and were used by Luria (1973):
Of utmost importance is the fact that all higher behavioral processes (or ‘higher cortical functions’) are really such complex functional systems, which are based on the coordinated functions (or ‘constellations’) of cerebral zones constructed in such a way that separate links of this system can be interchanged and that such a change does not affect the whole functional system. This approach is associated with a radical revision of the whole problem of ‘cerebral localization of functions’. We do not start with any attempts to ‘localize’ a complex function in a limited part of the brain; rather we try to discover how a ‘functional system’ is distributed in different parts of the brain, and the role that every part of the brain plays in the realization of the whole ‘functional system’. [29]
Luria thus never wholly associated functions with particular, isolated areas of the cerebral cortex, a view comparable to that of Wernicke, although he accepted the fact that different regions participated in different functions (he was therefore not a holist). Luria assumed that restoration of functions led to reorganization of a new and widely dispersed dynamic system and that it did not take place solely by transfer of function to equipotential brain areas. For details of his work and his many ideas and theories, the reader is referred to Luria’s autobiography [26] and the series of books he published, in particular Higher Cortical Functions in Man [32]. Luria had an enormous capacity for work and left hundreds of publications and dozens of books; he often had several jobs at once and was typically engaged in multiple scientific projects. In Luria’s obituary, Critchley (1978) described his visit to the Burdenko Institute:
To work as a visitor in his Burdenko Institute was a heady but exasperating experience. Oblivious to all sense of time, Luria seemed immune to such frailties as hunger and fatigue. He would move on from patient to patient, coping with one brash interruption after another. Discipline orderliness and regimentation were not there. His working conditions, let us face it, were astounding. Among the plethora of patients with brain trauma, Luria’s researches were carried out in an office which was more like a busy airport than the sanctum of a reflective scholar. Doors to the right and left of him opened and shut. Bells rang. All and sundry—nurses, technicians, porters, assistants—seemed to use his study like a public highway. Privacy there was none. Luria’s careful case studies were impervious to noise and distraction. [33]
In addition to his scientific, classical writings, Luria was also committed to what he himself called ‘romantic science’. This culminated in two books which Luria termed ‘biographical studies’—in fact, extensive case histories of men with ‘abnormal’ brain functions. One, the Mnemonist, is about Shereshevsky, a man who had an innate talent of remembering almost anything that he had experienced. He was able to recall near-infinite lists of words or sounds and repeat them years later. His synaesthetic memory (he described his recall as a journey through a remembered landscape) seemed to have no limits to its capacity nor durability. Characteristic of Luria is that he not only (thoroughly) researched Shereshevsky in a classical psychological manner, by measuring and testing his behaviour, but that he was also just as interested in how Shereshevsky’s strange condition affected his personality and his life. His brain seemed constantly involved in associations; those of new events and of those that he had earlier picked up in the outside world. These cerebral processes were virtually unstoppable and interfered with other brain functions, creating a downside to his incredible mnemonic talents. Shereshevsky had problems with more abstract concepts and personal relationships, and in the end, his ‘hypertrophied’ memory was probably more a curse than a gift. Remarkably, his memory also affected his behaviour in a more physical way:
He was able to control his involuntary processes, such as his heart rate and the temperature of his body, in the same way that a yogi does. A clear image of himself running fast increased his pulse rate. An image of a piece of ice on his hand decreased the temperature of his hand. And an image of his hand holding a glass of hot water increased his skin temperature. By this process he could increase or decrease the temperature of his hands by 5 degrees. [26]
The other book, The Man with the Shattered World, is about Zazetski, who as a young soldier was struck by a bullet in the left parieto-occipital region and was left with a myriad of neurological and psychological problems. Despite his visual disturbances, his amnesia and aphasia, Zazetski kept writing whenever he could, struggling for every word and sentence. He did so in an attempt to reconstruct his lost life and to recover the use of his damaged brain. Over a period of 20 years, Zazetski produced 3000 pages and this activity gave him, according to Luria, a reason to live. Luria edited these writings and added observations during the period of almost three decades in which he followed Zazetski in his clinic:
This book describes the damage done to a man’s life by a bullet that penetrated his brain. Although he made every conceivable effort to recover his past, and thereby have some chance of a future, the odds were overwhelmingly against him. Yet I think there is a sense in which he may be said to have triumphed. It is not false modesty on my part to wish no credit for this book. The real author is its hero.1
In letters to Oliver Sacks, who was a great admirer of his work and himself a master of ‘neurological novels’, Luria wrote (1973):
Frankly said, I myself like very much the type of ‘biographical’ study, such as Shereshevsky (the Mnemonist) and Zazetski … firstly because it is a kind of ‘Romantic Science’ which I wanted to introduce, partly because I am strongly against a formal statistical approach and for a quantitative study of personality, for every attempt to find factors underlying the structure of personality … only the style of these two books is different from the others; the principle remains the same. (…) I was ever conscious and sure that a good clinical description of cases plays a leading role in medicine, especially in Neurology and Psychiatry. Unfortunately, the ability to describe, which was so common to the great Neurologists and Psychiatrists of the 19th century … is almost lost now. [34]
For Luria, these case histories were as important as his scientific work. It shows his conviction that normal brain function is impossible without the integrity of the whole brain and the whole ‘personality’. To study and describe the nature of in particular the higher cognitive functions, Luria committed himself to two strategies:
The first was to trace their development; the second was to follow the course of their dissolution under conditions of local brain damage. In the mid-1920s Vigotsky first suggested that an investigation of localized brain damage could provide a way to analyze the cerebral structure and development of higher psychological processes. At that time, neither the structure of the higher psychological processes themselves nor the functional organization of the brain was clear. [26]
7.2.2 Aphasia
Around 1937, Luria turned his attention to ‘the tangled knot of disorders that were and still are referred to under the general rubric “aphasia”’ [26]. He began studying the three classes of aphasia that were at the time generally recognized: sensory, motor and semantic (or amnestic) aphasia. Luria used Pavlov’s fundamental idea of ‘nuclear zones’ and ‘systems of cortical analysers’ (see Fig. 7.4). Pavlov defined the nuclear zone as that part of the cortex that deals with the most precise differentiation and the most complex integration of special stimuli [26]. Within the centre of a zone lies the primary analyser. Examples are BA 17 in the visual zone, BA 21 in the auditory zone and BA 3 in the cutaneous–kinaesthetic zone. Primary analysers have a well-defined somatotopic projection for information that enters the cortex from the peripheral receptors, that is, proportional to their physiological importance (not their size). It corresponds to our current concepts of a primary cortical area. Luria noted that even these primary cortical areas already have a dynamic and not a static organization. He referred to the earlier investigations of Foerster and of Sherrington, whereby electrical stimulation of the same cortical point could lead to different functional responses. Luria also stressed that primary analysers already participated in the analysis of information and were not simply a representation of the peripheral stimuli:

Fig. 7.4
Diagram showing the interrelationship among fields of nuclear zones and analyser systems [129]. The nuclear zones (after Pavlov) consist of primary, secondary and tertiary analysers that deal with information that is subsequently more complex and multimodal [32]. These zones are denoted by circles (visual zone), squares (auditory zone), rhombi (general sensory zone) and triangles (motor zone); central fields within a nuclear zone are demarcated by larger symbols (note that numbers correspond to Brodmann areas). ‘The speech-motor (fields 44 and 45) and speech-auditory (back part of field 22) sections are identified by a slightly different shape of signs selected for the corresponding nuclear zones’ [129] (Figures and text from Neuron Structure of the Brain by Poliakov (1961, 1974) [32])
From the very beginning the sensory cortical divisions participate in the analysis and integration of complex, not elementary, signals. The units of any sensory process (including hearing) are not only acts of reception of individual signals, measurable in terms of thresholds of sensation, but also acts of complex analysis and integration of signals, measurable in units of comparison and discrimination. The sensory divisions of the cortex are the apparatuses responsible for this analysis, and indications of a lesion of these apparatuses are to be found, not so much in a lowering of the acuity of the sensations, as in a disturbance of the analytic-synthetic function. [32]
Secondary and tertiary zones were considered by Luria as ‘specifically human parts of hemispheres’: lesions within these areas do not generally result ‘in any elementary sensory or motor defects and remain inaccessible for classical neurological examination’ [29]. Secondary analysers occupy the periphery of the nuclear zones (e.g. the secondary auditory analyser is located in BAs 41, 42 and 22). Their cellular formation in the second and third layers of the cortex is more complex, allowing for more complicated operations [25]. Fibres from the thalamus also arrive in the secondary auditory zones, belonging to ‘the internal portion of the vertical connections transmitting impulses that have already been analysed and integrated’ [32]. Tertiary analysers are less modality specific and integrate information from different analysers.
To this cytoarchitectonic background, Luria added other anatomical studies, for instance, that of neuronographic investigations that showed connections of the secondary auditory zones in the temporal lobe to the inferior premotor cortex and frontal regions (Fig. 7.5). These connections established a functional network of anatomically distinct areas. ‘In this way, conditions are created for the auditory and motor analysers, especially those parts of the latter concerned with the innervation of the vocal organs, to work together’ [32].

Fig. 7.5
Schematic drawings of the brain showing connections between temporal and inferior frontal regions. Connections of each bundle of fibres with the cortex are denoted by identical numbers on the surface of the corresponding parts of the brain: (a) connections between the temporal lobe and inferior frontal gyrus and (b) connections between the temporal lobe and anterocentral gyrus (Luria reproduced this figure from Blinkov (1955) [130] and used it in his book Higher Cortical Functions in Man [32])
Luria once defined language as ‘the culturally determined syntactic systematization of signs and/or symbols’ [25]. His ideas on speech and language originated from several different scientific backgrounds. First, there was the obvious—but often forgotten—notion that language is important in communication and social interaction. This was the Vygotskian influence. In addition to that, Luria based his theories on neuroanatomical information and his own work in brain-damaged patients. A last important influence came from linguistics, which he studied at length in order to understand better the neural basis of language-related behaviour:
The two years I spent in the study of linguistics early in my career stood me in good stead when I began to work seriously on the problem of semantic aphasia because I could understand more fully the different mental requirements that seemingly similar linguistic acts placed on people. I was thus in a better position to carry out differential diagnosis of pathological symptoms which previously had been lumped together in the neurological literature. As my work continued to involve me in attempts to understand the brain basis of language-related behavior, I found it necessary to continue to study the psychology of language at the same time that I searched for its neurological bases. And just as advances in neurology and neurophysiology were instrumental to our study of brain mechanisms, advances in the study of linguistics were crucial to advancing our understanding of those phenomena of speech which brain pathology was interrupting; the two enterprises are inextricably bound together. Time and time again I found myself returning to old data, armed with new insights from advances in linguistics. [26]
Luria divided aphasia into general categories according to the subsystem of spoken language that is disturbed: phonetic, articulatory, semantic or dynamic. Vocate, in her book on Luria’s language research, remarks that these distinctions are predominantly for academic convenience as in practice they are much more difficult to distinguish because of ‘interdependent components of the functional systems of speech’ [25]. Both phonemic and articulatory aphasia are each subdivided into two types of aphasia, listing a total of six different syndromes. Luria related each of these aphasias to different regions of the brain and considered them neurologically different (Fig. 7.7). These different types of aphasia will be reviewed briefly below.
7.2.2.1 Phonemic (Sensory) Aphasia
For Luria, the basic difficulty underlying the symptoms of patients with classic sensory aphasia was ‘the inability to discriminate the distinctive features of phonemes, the basic units of word sounds’ [26]. Thus, in patients with a temporal lobe lesion, the difficulties in understanding words, naming objects, retrieving words or writing were secondary consequences of the primary defect in phonemic hearing [26]. Luria interpreted this disturbance of discriminative hearing as a ‘disturbance in the analytic-synthetic activity of the auditory cortex’ and regarded it as a fundamental symptom of a lesion in the posterior third of the left superior temporal gyrus (Fig. 7.6). He considered the resulting acoustic agnosia as the fundamental source of the speech disturbance, whereby disturbances could be divided into phonemic errors and conceptual errors [32]. Clinically, a patient with temporal aphasia typically has difficulty pronouncing a word that is heard, resulting in paraphasias (although paraphasias are not specific for the disorder). Disturbances of the motor aspect of speech may also be present. As the phonemic (sound) structure of speech is disturbed, it is ‘quite natural’, according to Luria, that the system of word meaning must also be disordered [32]. This was the second characteristic of sensory aphasia. ‘Often, only diffuse conceptual associations of the original meaning of the word remain, arising from the individual fragments of the sound complex’ [32]. Consequently, verbal comprehension will be impaired, the classic hallmark of sensory aphasia. The third essential part of temporal aphasia is disturbance in speech memory, invariably accompanying lesions in the superior temporal region:

Fig. 7.6
Schematic diagram of the distribution of cases (percentage) with impaired phonemic hearing as a result of traumatic lesions in different areas of the left hemispheres (Figure from Luria (1970) [28])
A disturbance of simple differentiation of audio verbal complexes, which arises as an inevitable result of temporal aphasia, causes words or groups of sounds similar in their acoustic composition to be no longer clearly distinguished, so that a person who normally could easily find the required name can no longer do so. Irrelevant acoustic complexes, which under normal conditions would have a very small chance of appearing during the perception of that particular object or the appearance of a given pattern, now appear just as probably as the appropriate words; the number of different acoustic complexes springing up in such a patient may often be so great that he is unable to pick out the required name, and the selectivity of the process of word finding is lost. [32]
Luria distinguished another type of temporal aphasia, namely, acoustic–amnestic aphasia. Such disturbances are the result of a lesion of the middle segment of the temporal lobe (i.e. the extranuclear divisions of the auditory analyser, BA 21 and 37). In contrast to the abovementioned acoustic–gnostic aphasia, in these cases phonemic hearing is largely preserved. Patients exhibit marked disturbances when they attempt to remember and reproduce words given to them orally (i.e. disturbances in verbal memory). They also cannot reproduce them in the proper order. To Luria, this ‘disturbance of the order of verbal traces is evidence of weakness of the tracer function of the cortex in this region’ [32].
7.2.2.2 Articulatory (Motor) Aphasia
A hallmark of motor aphasia is a disturbance in articulation. Again, this form of aphasia was not seen as a single syndrome by Luria, and he differentiated two main types. Luria referred to Bernstein, whose work demonstrated that correct performance of any motor act requires both efferent and afferent inputs:
By distinguishing between two components essential for the performance of a motor act—its kinesthetic basis, providing the differential composition of complex movements, and its kinetic structure, responsible for the formation of smooth skilled movements in easy consecutive order—a new approach in the analysis of the motor aspect of speech can be adopted and two different components (or two different forms) of motor aphasia can be described. [32]
The first type is afferent or kinaesthetic motor aphasia. This can be found in patients ‘with lesions in the lower parts of the posterior (kinaesthetic) parts of the left hemisphere’ [29]. In his book Language and Cognition, Luria specified this further to ‘the postcentral region of the speech region (Operculum Rolandi)’ [35]. The principle component is mispronunciation of individual speech sounds, which Luria called ‘articulemes’. The reason for this is that patients do not register feedback from the movements that are made to produce the articulemes. Therefore, movements lose selectivity and patients cannot assume the correct positions of the tongue and lips. These clinical features, Luria remarked, closely resemble a condition that had been described by German and French neurologists [29, 36, 37]. The second type of motor aphasia is efferent or kinetic motor aphasia. In these patients, articulation may be intact, but there are problems with the transition from one articuleme to another. Their ‘kinetic melody’ is disturbed. These patients have lesions within the lower part of the left premotor cortex, the classic Broca’s area.
7.2.2.3 Semantic (Amnestic) Aphasia
In this form of aphasia, patients have a good understanding of the meaning of individual words, but they cannot grasp the meaning of more complex ideas. Characteristic is disturbances of logico-grammatical relations, whereas there are rarely signs of disturbed articulation or phonemic hearing (i.e. no sensory or motor deficits). ‘Such patients find it almost impossible to understand phrases and words which denote relative position and cannot carry out simple instructions such as “draw a triangle above a circle”’. Head had described in 1926 that there were accompanying difficulties in the perception of complex spatial relations. The syndrome is caused by lesions that extend within the temporoparietal-occipital (‘tertiary’) area. That is why, according to Luria, ‘the syndrome of “semantic aphasia” includes, as a rule, deterioration of orientation in space, constructive apraxia, and defects in computation’ [29].
7.2.2.4 Dynamic Aphasia
In these patients spontaneous and original speech is severely reduced, while naming, repetition of words or even simple sentences is preserved. When required to tell a story, patients complain of an ‘emptiness in the head’ [28]. There is doubt to what extent syntactic and grammatical processes are affected, as Luria only provided qualitative descriptions of patients with dynamic aphasia [38]. Luria referred to pioneering investigators who had described this syndrome, notable Lichtheim’s transcortical motor aphasia [29]. The lesion is located anterior to Broca’s area, in the ‘tertiary zone’. Current opinion does not agree on any specific frontal region nor on its underlying mechanism [38, 39].
Figure 7.7 shows an abstraction of the localization of the different types of aphasia that were considered by Luria. Graphically, at least, the model has similarities to the Wernicke–Lichtheim model. However, there are crucial differences, as formulated by Tesak and Code (2008):

Fig. 7.7
Luria’s classification of the location of lesions that produce different types of aphasias. (1) Dynamic aphasia, (2) efferent motor aphasia, (3) afferent motor aphasia, (4) sensory aphasia, (5) acoustic–amnestic aphasia and (6) semantic aphasia (Figure from Kagan and Saling [131])
First, he [Luria] emphasizes the individual processes (analysis, synthesis, integration) engaged in language; his is a process model. Second, the possibility of aphasic symptoms being connected at different linguistic levels on the basis of abstract principles is implied in Luria’s work. The disturbance of the linear scheme, which shows itself in sound production, sentence production and in writing is an example. Third, Luria’s process model provides routes for the formulation of strategies for rehabilitation, because the model is flexible and dynamic in contrast to the static classical model and because the brain is conceptualized overall as an interactive system. [1]
Luria certainly was ahead of his time by anticipating that clinical, cognitive and anatomical studies need to be integrated to enhance our understanding of brain–behaviour relationships. Even now, his work is of much inspiration and importance [40]. Luria’s theoretical concepts of distributed and dynamic functional systems, for instance, remain highly relevant in our era of modern neuroimaging. Although our new techniques are powerful and provide us with detailed maps of structural and functional connectivity within individuals, their use often seems more data-driven than guided by predictive theoretical models.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


