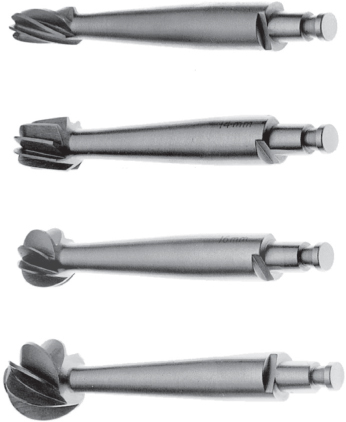
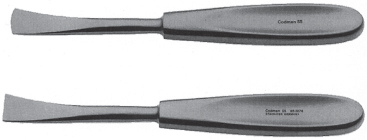
15 All surgical instrument images were reproduced with permission from Codman and Shurtleff, Inc. All rights reserved. Fig. 15.1 Adson forceps. Adson forceps are used to lift the skin without trauma to the tissues. Ensure the tissue is not tightly grasped, which may injure or necrose the skin after closing. One trick is to “lift” the skin from inside out rather than “pinching it.” As with all surgical instruments, the surgeon must remain aware of the pressure exerted on the tissue by the forceps and adjust the closing pressure accordingly. Fig. 15.2 Penfield watchmaker forceps. Penfield watchmaker forceps are typically used for delicate tissues such as the dura or structures in which distal teeth may cause injury. Frequent used for dural closure. Fig. 15.3 Gerald dressing forceps. Gerald dressing forceps are favored by many because they tend to be less traumatic to the tissue than toothed forceps. Some people like to use these when closing skin instead of Adson forceps. They can also be utilized to manipulate dura when opening or closing. Fig. 15.4 Raney scalp clip applying forceps. Raney clips are placed on the scalp for hemostasis. Place them no more than 1 cm apart except in redo operations, where the tissue may already be prone to ischemia. Use only as many Raney clips as necessary to achieve the desired hemostasis. Too many clips on ischemic or previously radiated scalp can result in poor wound healing. Fig. 15.5 Gigli saw handles. The Gigli saw is used to create an opening in the bone (craniotomy). It was the original instrument used before the advent of the high-speed drill. It is still used nowadays in certain areas difficult to reach with the drill, such as the supraorbital rim. When using the Gigli saw, it is useful to start slowly, allowing the saw to engage and progress in speed. It is also important to use ample long movements keeping the saw blade as straight as safely possible, usually by providing maximal distance between hands. Fig. 15.6 Gigli saw guide. Passed from one burr hole to another with the Gigli wire attached. For close burr holes, use a Kerrison bone punch to bevel openings to prevent contusion secondary to a deep curve of the Davis guide. Always remember that the brain resides just underneath the dura. Fig. 15.7 Gigli wire saw. Used for large, accurate craniotomy cuts in the fronto-orbital region by some surgeons. Since the advent of pneumatic and electric drills, it is possible that students and residents may never see a Gigli saw used on a craniotomy. Remember that the saw should glide through the bone like butter. If it binds up, then the operator may be applying too much pressure. Fig. 15.8 Hudson brace. The Hudson brace allows slow, methodical rotation, providing dexterity and unparalleled control without walking or plunging. As with the Gigli saw, the advent of pneumatic and electric drills may mean that the student may never see a Hudson brace. Always nice to have around, just in case the power goes out. Fig. 15.9 Hudson burrs. A variety of bits are available for use with the Hudson brace. Fig. 15.10 Cushing periosteal elevators: rounded edge and square edge. Periosteal elevators are used frequently after incising the skin during a craniotomy flap to retract the periosteum. These are very useful for subperiosteal dissection of the temporalis muscle. Often used as retractors on cranial cases. Fig. 15.11 Woodson elevator. Woodson elevators are used to dissect the dura off the bone on craniotomies. It is also used in lumbar spine cases to check for the location of the exiting nerve root canal and pedicle. Some surgeons call this instrument the “dental tool” or “hockey stick.” Fig. 15.12 Mastoid retractor.
Neurosurgical Instruments
Acknowledgment for Images Used










Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Neurosurgical Instruments
Only gold members can continue reading. Log In or Register to continue




