• Subperiosteal exposure of the occiput and the C1–C2 vertebral levels is essential for instrumentation placement.
• The vertebral artery travels along the superior lateral surface of the C1 arch approximately 1.5 cm from the midline.
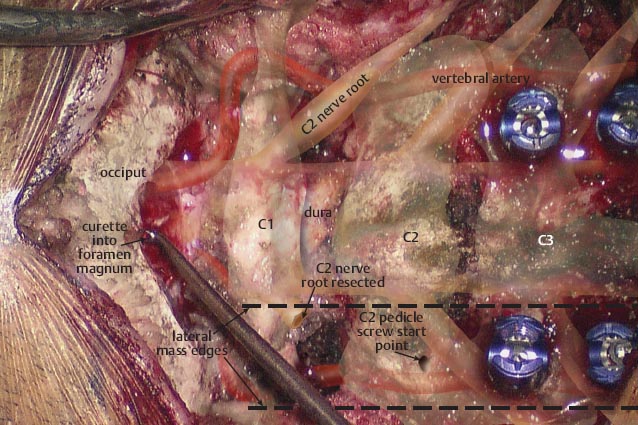
• A curette is placed into the foramen magnum to clearly define the inferior border of the occiput.
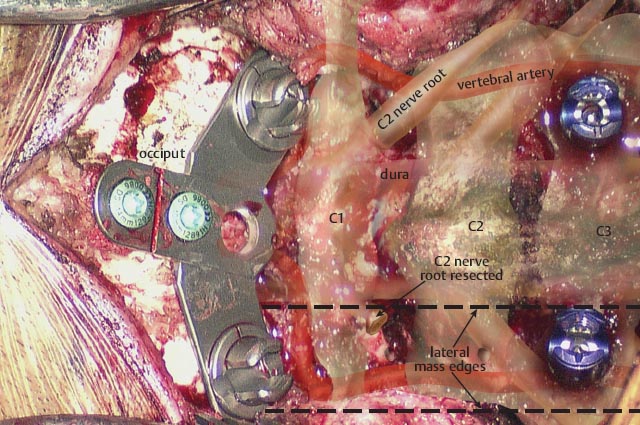
• An occipital plate has been applied. Screws are placed bicortically in the midline.
– The plate is appropriately sized so that it is easier to connect the occipital and C1–C2 screw tulips.
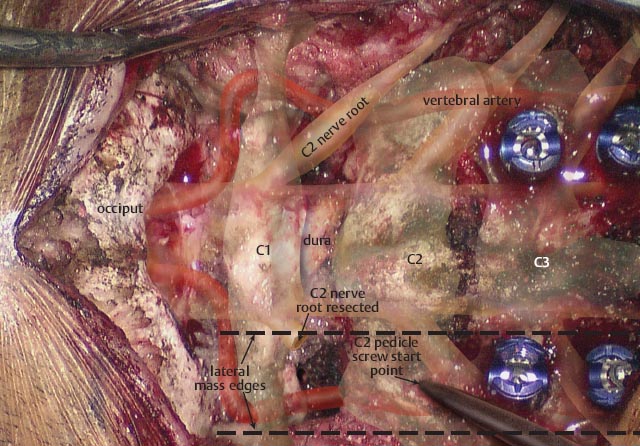
• The C2 (axis) pedicle screw starting point occurs at the inferior and lateral edge of the inferior articular process of C2.
– The vertebral artery lies directly anterolateral. The screw should be directed medial and cephalad to avoid potential vascular injury.
 Screws placed bicortically into the anterior axis may risk injury to the internal carotid artery.
Screws placed bicortically into the anterior axis may risk injury to the internal carotid artery.
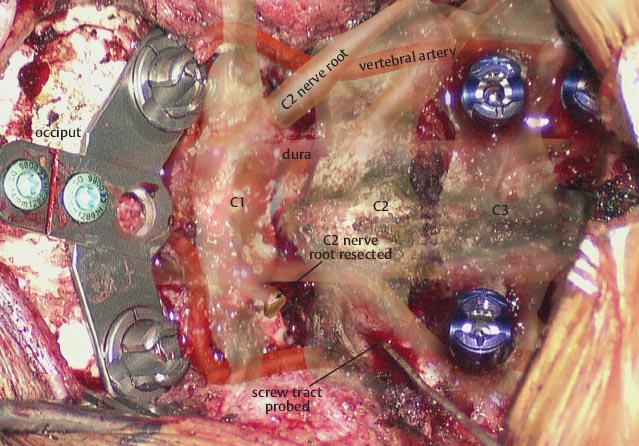
 The C2 screw is angled 20° medially and 15–20° caudally (use lateral flouroscopy).
The C2 screw is angled 20° medially and 15–20° caudally (use lateral flouroscopy).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


