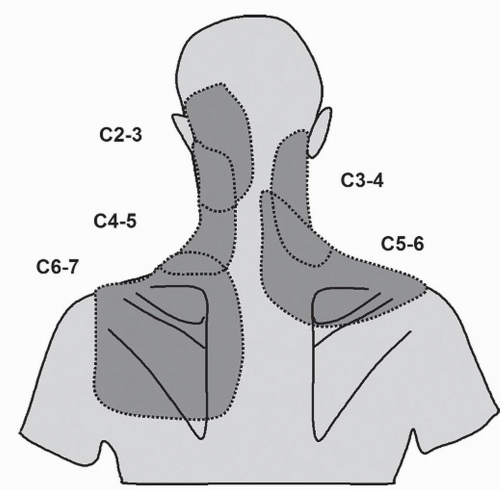
 Figure 19.1. Maps of the distribution of somatic referred pain following noxious stimulation of the cervical zygapophysial joints at the segmental levels indicated. |
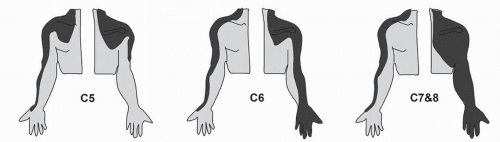 Figure 19.2. Maps of the distribution of cervical radicular pain from commonly affected segments. |
TABLE 19.1 The Proportions of Patients Showing Different Degrees of Relief from Cervical Radicular Pain Following Cervical Epidural Steroid Injections | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
treatment, the proportions of patients achieved greater than 75% relief or between 50% and 74% relief of pain after epidural steroids were not significantly greater than the corresponding proportions after intramuscular steroids, but the combined proportion of patients achieving at least 50% relief is greater for epidural steroids (Table 19.2). At 1 year after treatment, the proportions of patients achieving at least 75% relief and greater than 50% relief significantly favor epidural steroids.
TABLE 19.2 The Numbers and Proportions (95% Confidence Intervals) of Various Grades of Relief Achieved in a Controlled Trial of Cervical Epidural Steroids and Intramuscular Steroids for Cervical Radicular Pain | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
(34, 35, 36 and 37). The prevailing view is that if injected into a radicular artery, or into the vertebral artery, particulate steroids act as emboli and cause spinal cord or brainstem infarction. The incidence of such complications is not known, but at least 78 cases have been recorded in the literature (34). Some exponents of the procedure have reported no instances of neurologic complications in 1,063 patients, and only minor complications in 1.6% of cases (38). Implicitly, serious complications are rare, but they are devastating in nature. Ironic is that fact that steroids have been implicated as the offending agent, yet steroids have been shown to be redundant for the small success rate of this procedure.
Related posts:
 Developmental Anatomy of the Normal Cervical Spine
Developmental Anatomy of the Normal Cervical Spine
 Neurologic Examination: Grading Scales
Neurologic Examination: Grading Scales
 Cervical Spine Injuries in Children
Cervical Spine Injuries in Children
 Calcification of the Ligamentum Flavum of the Cervical Spine
Calcification of the Ligamentum Flavum of the Cervical Spine
 Artificial Disk Surgery of the Cervical Spine: Contraindications for Cervical Disk Arthroplasty
Artificial Disk Surgery of the Cervical Spine: Contraindications for Cervical Disk Arthroplasty
 Controversies, Myths, and Realities Regarding the Surgical Treatment of Cervical Spondylotic Myelopathy with a Special Focus on Laminoplasty
Controversies, Myths, and Realities Regarding the Surgical Treatment of Cervical Spondylotic Myelopathy with a Special Focus on Laminoplasty
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


