Figure 19-1 Serial transverse paraffin sections. A, Hematoxylin and eosin section demonstrates multiple whorl-like structures corresponding to microfascicles (arrow) replacing the normal architecture of the nerve. Note one preserved nerve fascicle (arrowhead). B, Epithelial membrane antigen (EMA) preparation demonstrates reactivity of the microfascicle walls, confirming their perineurial origin. C, S-100 preparation shows reactivity of Schwann cells and fibers within microfascicles.
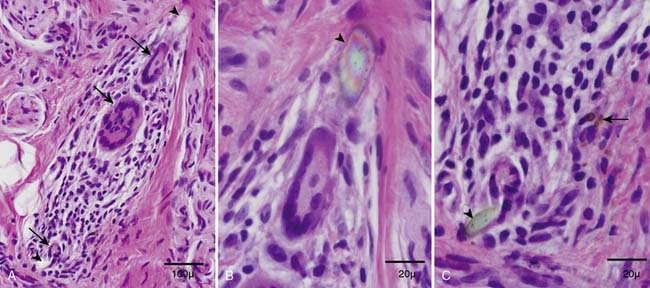
Figure 19-2 A, Hematoxylin and eosin transverse paraffin section shows three multinucleated giant cells (arrows) admixed with a moderate lymphocytic infiltrate. Note that when the lower and upper tips (arrowheads) of the inflammatory infiltrate are magnified and observed under polarized light (B and C), the multinucleated giant cells are in close proximity (B) or in contact (C) to foreign bodies with birefringent properties. Note hemosiderin deposits (arrow) neighboring one foreign body (C), presumably from trauma. These findings confirm a foreign body inflammatory reaction presumably to suture material.
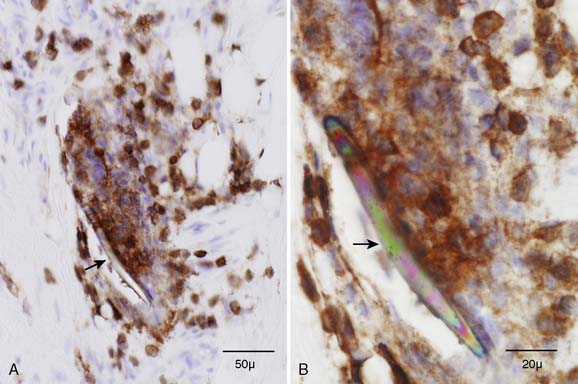
Figure 19-3 A, A transverse paraffin section demonstrates a moderate inflammatory infiltrate that reacts to a leukocyte common antigen (CD45) preparation. B, Magnification of the same section under polarized light shows a linear foreign body (arrow) with rainbow-like colors within the inflammatory infiltrate.
CONCLUSION
We present a case of painful injury neuroma occurring after inadvertent partial transection of the sural nerve during removal of a ganglion cyst. The biopsy revealed unexpected lymphocytic infiltrates, multinucleated giant cells, and hemosiderin deposits in addition to the classic histopathologic findings of an injury neuroma. The use of polarized light clarified the source of the granulomatous reaction and bleeding within the injury neuroma. We postulate that the traumatic suturing of the proximal nerve stump and the secondary foreign body reaction played a major role in the formation of a painful injury neuroma.
Foreign body reaction from suture material can stimulate excessive scarring after suture repair of peripheral nerves.2 Tumor necrosis factor (TNF) and interleukin-1 (IL-1) are known mediators of tissue injury and foreign body reactions. Macrophages and T cells invading nerves release TNF and IL-1 which stimulate the local non-neuronal cells to produce nerve growth factor (NGF).3 NGF is trophic to sensory and sympathetic fibers during nerve regeneration but may also play a role in the pathogenesis of injury neuroma and neuropathic pain.4 The mechanical hyperexcitability of regenerating nerve sprouts trapped in the neuromas, potentially explaining neuroma tenderness, is attributed to change in phenotype, quantity, and distribution of sodium ion channels of neuroma afferents,5,6 probably in part due to NGF excess.7 The chronic inflammation from suture granuloma of the proximal nerve stump in our patient likely led to a relative excess of TNF, IL-1, and NGF, and created a milieu favorable for the formation of a painful neuroma.
Intraneural perineurioma and injury neuroma can share similar morphologic (focal nerve enlargement) and histopathologic features (whorls of concentric perineurial cells encircling myelinated fibers). There is controversy regarding the true nature of perineurioma. The rare occurrence of perineurioma at entrapment sites suggests a reactive process.8 However, clonal abnormalities found on chromosome 22 suggest a true neoplasm and not a reactive process.9 Diffuse microfasciculation beyond the perineurium of the original nerve fascicles into the epineurium with marked disruption of nerve architecture is typical of injury neuroma. Endoneurial microfasciculation with expansion of nerve fascicles but relative preservation of original perineurium and nerve architecture is typical of perineurioma.
Standard light microscopic examination of the patient’s injury neuroma showed multinucleated giant cells and lymphocytic infiltrates, but the suture material was not obvious. Suture material became conspicuous with polarized light because of its strong birefringence. Painful injury neuromas due to foreign body reaction are probably under-recognized because polarized light microscopy is not routinely used for evaluation of inflammatory infiltrates in nerve biopsies. We recommend its routine use in nerve biopsies that show a granulomatous reaction.
Related posts:
 An Unusual Case of Pia-Arachnoiditis due to Metastatic Breast Carcinoma
An Unusual Case of Pia-Arachnoiditis due to Metastatic Breast Carcinoma
 Stepwise Facial and Upper Limb Weakness and Small Fiber Sensory Loss—Tangier Disease
Stepwise Facial and Upper Limb Weakness and Small Fiber Sensory Loss—Tangier Disease
 Focal Mononeuropathy Onset of Amyotrophic Lateral Sclerosis
Focal Mononeuropathy Onset of Amyotrophic Lateral Sclerosis
 Meningeal Enhancement in POEMS Syndrome: Another Clinical Sign of Vascular Endothelial Growth Factor Overactivity?
Meningeal Enhancement in POEMS Syndrome: Another Clinical Sign of Vascular Endothelial Growth Factor Overactivity?
 POEMS Syndrome
POEMS Syndrome
 Amyloidosis Typing Based on Laser Microdissection and Mass Spectrometry of Paraffin-Embedded Tissue Biopsies
Amyloidosis Typing Based on Laser Microdissection and Mass Spectrometry of Paraffin-Embedded Tissue Biopsies
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


