50 Parasitic and Fungal Disorders and Neurosarcoidosis
Cerebral Malaria
Clinical Vignette
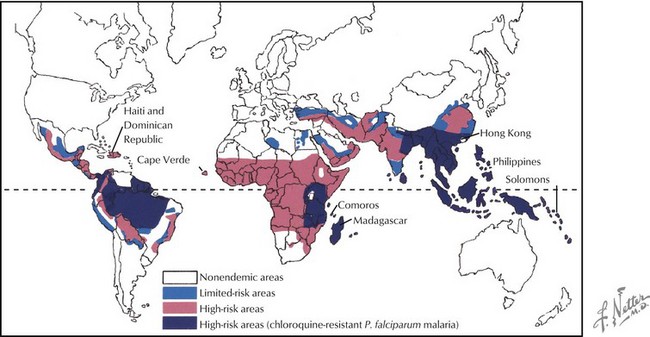
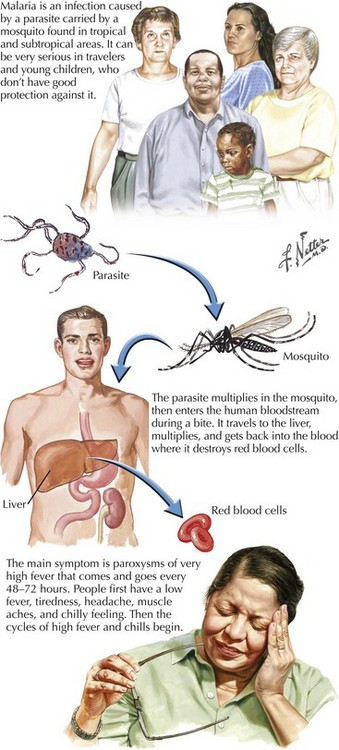
Malaria continues to have a global presence, primarily affecting individuals living in South and Central America, Africa, and Asia (Fig. 50-1). Close to a half billion individuals are affected annually with up to a million deaths each year. Previously endemic in the United States, public health measures have greatly decreased its incidence here. However, at least a thousand cases are reported annually here and are primarily related to P. falciparum affecting travelers to endemic geographic areas.
Therapy
Increased drug resistance has led to combination therapy for malaria. The treatment of cerebral malaria consists of either intravenous quinidine or artesunate accompanied by doxycycline (Fig. 50-2). Intravenous quinidine has to be administered in an ICU setting with electrocardiographic monitoring, as it may lead to severe arrhythmias. Exchange transfusion should be strongly considered for persons with a parasite density of more than 5–10% or even with a lower level of parasitemia if the cerebral malaria is severe or other complications of the malaria occur, including non–volume overload pulmonary edema, or renal complications.
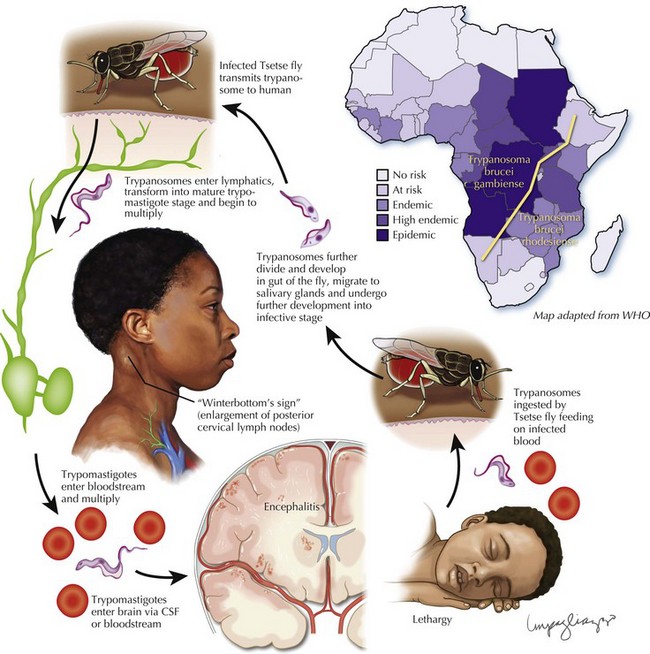
African Trypanosomiasis (Sleeping Sickness)
Clinical Features
Once the neurologic manifestations emerge, the patient often has developed an advanced stage of central nervous system (CNS) infection. Personality changes are common; patients are frequently mistaken as having psychiatric disorders, as in this case. In the early phases of CNS disease, a disruption of the normal circadian sleep rhythm occurs (Fig. 50-3).