• A midline posterior approach is utilized, with dissection performed through the avascular ligamentum nuchae.
• Subperiosteal exposure is performed, extending out to the lateral edge of the lateral mass.
– Bleeding is typically encountered along the lateral edge of the lateral mass.
– This bleeding can be controlled with bipolar cautery.
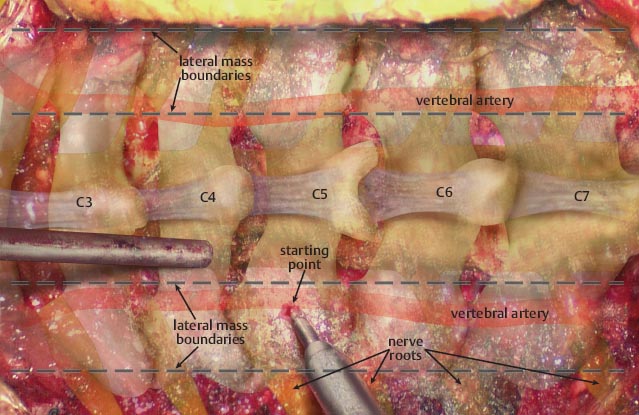
• The lateral mass is exposed and clearly defined, exposing the superior, inferior, and medial lateral borders.
• Once the lateral mass is defined, the starting point should be created with a high-speed burr.
– The center of the lateral mass is burred first.
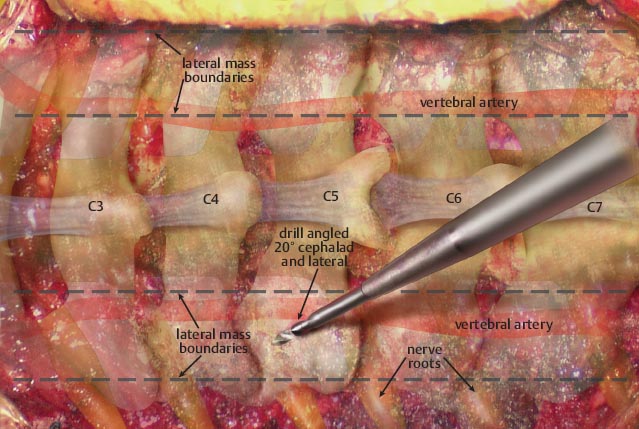
– The drill is then directed 20° cephalad and lateral, thereby avoiding the vertebral artery and nerve root.

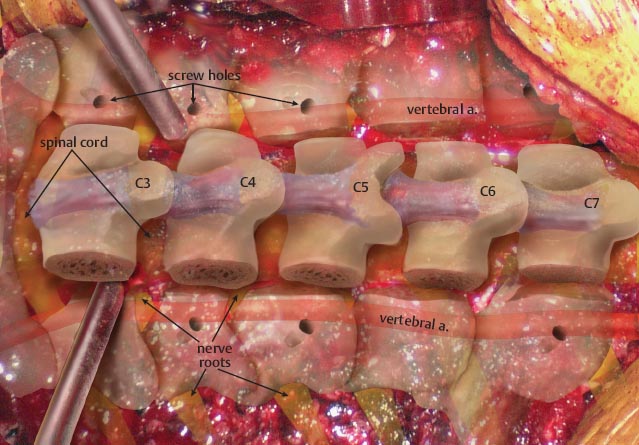
• Once the lateral mass screw holes are created, a laminectomy can be performed.
– Two troughs are created with a high-speed burr.
– The troughs are created just medial to the screw start points at the junction of the lateral mass and lamina.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


