Disablement involves the complex relationship between disease, impairment, disability, and handicap.
Functional disabilities are targeted in neurorehabilitation.
Neurorehabilitation encompasses medical, physical, social, educational, and vocational interventions provided in institutional or community settings.
Ongoing and thorough patient assessment is crucial throughout the neurorehabilitation process.
Rehabilitation goals and the management plan are regularly assessed and modified when necessary to maximize patient potential.
Patients having disabilities due to an acute, chronic, or progressive neurologic condition may benefit from neurorehabilitation.
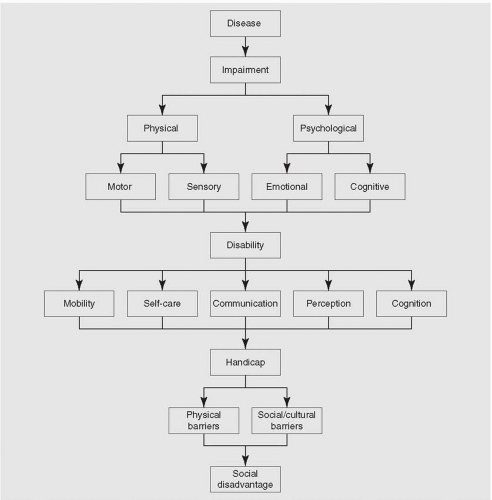
The World Health Organization has described disablement in terms of disease, impairment, disability, and handicap (Table 27.1). In this conceptual model, disease is an underlying condition or pathologic process that results in an impairment. Impairment is an abnormality in physical or psychological capacity. Disability is the limitation an impairment places on an individual’s ability to perform necessary routine daily functional activities. Handicap is the social disadvantage that results from disabilities that prevent an individual from fulfilling his or her expected role in society. Handicap is influenced in a society by physical barriers, social and cultural factors, and the attitudes of those involved (Fig. 27.1).
TABLE 27.1 Aspects of Disablement
Disease: a condition or pathologic process that may result in an impairment
Impairment: an abnormality in physical or psychological capacity
Disability: limitations in function resulting from an impairment
Handicap: social disadvantages that result from disabilities
FIGURE 27.1 Process of disablement
▪ SPECIAL CLINICAL POINT: A host of neurologic conditions that may be developmental, hereditary, infectious, autoimmune, metabolic, degenerative, vascular, neoplastic, or traumatic exist that can result in static or progressive impairments.
Neurologic disorders can occur at any point in an individual’s lifetime and the pathology may involve any part of the nervous system, from the central nervous system (CNS) (including the brain or spinal cord) to the peripheral nervous system and the muscle (resulting in impairments such as disorders of strength, endurance, balance, coordination, mobility, cognition, perception, communication, swallowing, and sensation). The same neurologic impairments can vary in intensity among individuals depending on the pathologic cause or the region of the nervous system affected. Similarly, the prognosis may differ with similar impairments but with different pathologic processes at work. For example, hemiparesis resulting directly from an area of brain infarction would be less likely to resolve than would hemiparesis resulting from demyelination or edema involving the same region of the brain.
Disabilities that may result from neurologic impairments can involve mobility, self-care, communication, cognition, and perception. Deficits of mobility may include problem with bed mobility, transfers, and ambulation. Deficits of self-care may include problems with any of the routine daily functions of an individual from ordinary self-care tasks, including grooming, toileting, bathing, dressing, and feeding, to the more complex tasks of independent living, including financial management, shopping, home making, and the ability to use a telephone or drive a car. Pathology at different sites of the nervous system can result in similar functional disability manifestations between individuals. For example, disorders affecting balance, coordination, cognition, or strength all may separately result in the inability of an individual to walk or to effectively perform routine self-care activities.
▪ SPECIAL CLINICAL POINT: In neurorehabilitation, functional disabilities are the focus of medical, restorative, adaptive, environmental, and social interventions.
Neurorehabilitation encompasses medical, physical, social, educational, and vocational interventions that can be provided in a variety of institutional and community settings. Professionals include specialized physicians, nurses, therapists, psychologists, social workers, dietitians, and orthotists. Goals include the prevention of secondary complications, treatment to reduce neurologic impairments, compensatory strategies for residual disabilities, patient and caretaker education, and maintenance of function (Table 27.2). Anyone with neurologic impairments can benefit from neurorehabilitation, but the setting, approach, and limitations of treatment will vary with the type and extent of the disabilities. The objective is to match patient needs with capabilities of available programs. This chapter will focus on principles of neurorehabilitation, including a broad overview of the role of ongoing patient assessment, acute-care intervention, the determination of rehabilitation need and an appropriate setting, the rehabilitation management plan, and issues pertaining to community transition and neurorehabilitation outcomes. In addition, case presentations will be given in the Questions and Discussion section to explore potential benefits and limitations of neurorehabilitation in a variety of neurologic conditions.
TABLE 27.2 Goals of Neurorehabilitation
Treatments to reduce neurologic impairments
Compensatory strategies for residual disabilities
Prevention of secondary complications
Maintenance of function
Patient/caretaker education
ROLE OF ASSESSMENT IN NEUROREHABILITATION
Ongoing and thorough patient assessment is a crucial aspect of the neurorehabilitation process. The goals of assessment change over the clinical course of rehabilitation from the acute hospitalization, to the transfer to a rehabilitation facility or program, to the transition back to the community. Initial concerns often include patient survival, level of consciousness, and response to acute treatments. Later concerns focus on specific neurologic impairments and a patient’s functional abilities.
▪ SPECIAL CLINICAL POINT: Patient evaluation throughout the neurorehabilitation process involves clinical examinations and well-validated standardized measures performed by various members of the interdisciplinary team of rehabilitation specialists.
This team often is composed of the physician (neurologist or physiatrist), nurses, a social worker, therapists (including physical, occupational, speech, and recreational/vocational), and a psychologist.
The non-neurologist primary care physician will likely benefit from a neurorehabilitation consultation for evaluation of all patients admitted to the hospital with acute neurologic impairments resulting in functional deficits. In addition, patients with chronic medical or neurologic conditions with functional deficits that may be related to deconditioning weakness, reduced joint mobility, or progression of the condition also may benefit from rehabilitation. In principle, a neurorehabilitation evaluation should be obtained for all hospitalized or ambulatory clinic patients with functional decline in any routine daily functions including mobility; transfers; ambulation; or the ability to dress, bathe, feed, groom, speak, or carry out previously routine duties such as vocational or homemaking responsibilities.
The objectives of neurorehabilitation assessment during the acute hospital admission include documentation of the diagnosis, the impairments, and the disabilities as well as identification of treatment needs. Subsequent reevaluation focuses on response to acute-care treatments and any changes in neurologic or medical status. Once patients are medically stable, the evaluation is geared toward identifying those who will benefit from further rehabilitation intervention and determining the appropriate rehabilitation setting. Recommendation may be made for referral to an interdisciplinary rehabilitation program, in an inpatient or an outpatient facility, or for selected individual rehabilitation services in an ambulatory care setting.
On admission to a neurorehabilitation program, assessment is performed to help develop a rehabilitation management plan with realistic goals and to document a baseline level of function for monitoring progress. Periodic weekly or biweekly reassessment during the rehabilitation program allows patient progress to be monitored, treatment regimens to be adjusted when necessary to maximize patient potential, and discharge planning to be facilitated. Objectives of assessment after discharge include the evaluation of patient adaptation to the home environment and community setting, the determination of the need for further rehabilitation services, and the assessment of caregiver burden and needs.
Standardized assessment instruments in neurorehabilitation complement the neurologic examination in evaluating functional recovery. Standardized measurement scales facilitate reliable documentation of severity of functional disabilities, help to increase consistency of treatment decisions, facilitate communication between therapists, and provide a reliable basis for monitoring progress. Scales exist to measure many areas of neurologic function, such as consciousness, cognition, perception, communication, strength, mobility, balance, coordination, somatosensation, and affective function. For example, the Rancho Los Amigos Cognitive Scale often is used to document levels of cognitive recovery following a traumatic brain injury, and the Functional Independence Measure Scale often is used to assess levels of independence in areas of basic daily function. In addition, many other scales exist to help measure and quantify specific functional impairments and disabilities. Limitations of various standardized measurement scales often are counterbalanced by use of other scales and the neurologic examination.
Another important aspect of patient assessment in neurorehabilitation is the clarification of the complex relationship that exists between disease, impairment or severity of objective deficits, and disability or the impact of disease on function in any individual patient.
Specific neurologic impairments may play a role in multiple functional disabilities. For example, a patient’s inability to adequately selffeed, dress, or propel a wheelchair could separately result from impairments in strength, endurance, cognition, comprehension, perception, sensation, coordination, balance, lack of motivation, or the presence of pain or fatigue. Furthermore, individual impairments may have multiple possible etiologies. For example, fatigue may result directly from a neurologic disease process or it may indirectly result from depression, sedative side effects of various medications, or a lack of adequate sleep. Similarly, a patient’s inability to effectively concentrate and attend to therapies may result from impairments of cognition or perception resulting directly from neurologic disease or indirectly from depression, the side effects of medications, or the distraction of pain. Thus, the role of assessment in neurorehabilitation includes clarification of etiologies contributing to a patient’s disabilities so that appropriate therapeutic interventions may be undertaken at any point during the rehabilitation process. In addition, certain treatments may be contraindicated or recovery may be limited by comorbid chronic conditions such as cardiovascular disease, chronic pulmonary disease, cancer, musculoskeletal disorders, or psychiatric conditions. Evaluation and treatment of poorly controlled comorbid medical conditions also will improve neurorehabilitation outcomes.
Neurorehabilitation During Acute Care
▪ SPECIAL CLINICAL POINT: Neurorehabilitation intervention should begin following an acute hospitalization once a neurologic diagnosis has been established and life-threatening problems are controlled. Highest priorities are the prevention of secondary complications, maintenance of general health functions, early mobilization, and resumption of self-care activities (Table 27.3).
Immediate neurorehabilitation concerns include the maintenance of homeostasis and the prevention of complications that could result from the particular neurologic condition. Maintenance of homeostasis is a priority in all neurologic patients in the acute-care hospital setting. Routine continuous monitoring of basic health functions can help to prevent further disability. Included in any rehabilitation program are efforts to ensure regulation and adequacy of nutrition and hydration, bladder and bowel function, and sleep. In addition, measures usually are undertaken to prevent deep vein thrombosis (DVT), pulmonary embolism, skin ulcerations, orthostasis, development of joint contractures, and pneumonia, which all may result from impaired mobility. In those patients with disorders of swallowing or cognition, efforts also are undertaken to prevent malnutrition and dehydration. The prevention of recurrent stroke is a concern in those individuals with acute cerebrovascular disorders. Autonomic dysreflexia is of concern in individuals with spinal cord injury or disorders. Autonomic dysfunction including cardiovascular dysfunction is of concern in patients with the acute Guillain-Barré syndrome (acute demyelinating polyneuropathies). In addition, efforts to prevent falls and accidental fractures or joint dislocations are undertaken in all patients who may be at risk.
TABLE 27.3 Neurorehabilitation during Acute Care
Prevention of secondary complications
Deep vein thrombosis/pulmonary embolism
Skin breakdown
Joint contractures/dislocations/subluxations
Pneumonia
Falls
Autonomic dysfunction
Malnutrition/dehydration
Maintenance of homeostasis
Normalization of sleep
Normalization of bowel/bladder function
Normalization of nutritional states
Promotion of early mobilization and return to self-care
Maintenance of Homeostasis
Dehydration and malnutrition may be consequences of neurologic disorders resulting in dysphagia, inability to self-feed, confusion, or inability to communicate hunger or thirst. Reduction of risk may include monitoring daily intake of liquids and calories, weekly determinations of body weight, and supervision with meals. A formal dysphagia assessment may be indicated in certain patients (see Management of Dysphasia and Aspiration, below).
Bladder dysfunction is another possible consequence of neurologic disease. Bladder dysfunction may result from neurologic conditions causing bladder hypertonicity, bladder hypotonicity, and areflexia or hyperactivity of the internal or external sphincters. Often, a urologic consultation and urodynamic testing is necessary. Treatment may involve a program of bladder training that may include intermittent bladder catheterization, certain medications, and toileting at regular intervals. Use of indwelling Foley catheters is avoided with the exceptions of urinary retention that cannot otherwise be controlled, in patients with extensive skin ulcerations, or if incontinence interferes with fluid and electrolyte balance monitoring.
Bowel dysfunction, and particularly constipation or fecal impaction, may occur in neurologic disease as a result of immobility, inadequate nutrition (food or fluid), cognitive impairment, neurogenic bowel, and even depression or anxiety. Treatment measures include the assurance of adequate intake of fluids and fiber, establishment of a regular toileting schedule, and judicious use of stool softeners or laxatives.
Insomnia may occur as a direct result of a neurologic disorder, or it may result indirectly from comorbidities including depression, agitation, anxiety, the side effects of medications, muscle spasms, pain, inability to move in bed, urinary frequency or incontinence, or interruptions related to the hospital environment. Inadequate sleep can result in daytime drowsiness and inability to fully benefit from rehabilitation therapies. Goals of management include determination and treatment of a specific etiology if one exists; alteration of the environment if necessary to reduce disturbances of sleep; adjustment of type, timing, and dose of offending medications; and if all else fails, limited judicious use of hypnotic medications.
Prevention of Deep Vein Thrombosis
Acute prolonged immobility, and particularly the paralysis of one or both legs, places an individual at risk for deep vein thrombosis (DVT) and pulmonary embolism. Randomized trials have shown effective risk reduction with use of subcutaneous low-dose heparin or low-molecular-weight heparin products. In addition, warfarin, intermittent pneumatic compression, early mobilization, and elastic stockings have been shown to be effective. Management of DVT risk in neurorehabilitation often includes early mobilization; elastic stockings; and, in the absence of contraindications, mini-dose subcutaneous heparin.
Prevention of Skin Breakdown
Risk factors for skin breakdown include impaired cognition, poor mobility, incontinence, spasticity, and obesity. Steps to maintain skin integrity in those at risk include systemic daily inspection, gentle routine skin cleansing, protection from moisture, maintenance of hydration and nutrition, efforts to improve patient mobility, frequent turning and repositioning of immobile patients, and avoidance of skin pressure or friction. Prior to discharge from the acute-care hospital setting, patients or caretakers should be educated on skin care issues.
Prevention of Joint Contractures
A patient’s potential for functional recovery may be limited by the restriction of movement or pain that results from joint contractures. The joints of spastic paretic limbs are most at risk for contractures. Simple prolonged disuse of an extremity also can result in contractures. For example, a comatose individual with spastic hemiparesis is at risk for bilateral plantar flexion contractures, with one plantar flexion contracture related to spasticity and the other related to simple disuse. Spasticity often develops in individuals with so-called’upper motor neuron lesions” that result from disorders involving the brain or spinal cord. Spasticity may involve one extremity (monoparesis) to all four extremities (quadriparesis), depending on the underlying pathologic process.
▪ SPECIAL CLINICAL POINT: Routine prevention of contractures often includes antispastic limb positioning, frequent range-of-motion exercises with passive or active stretching, and splinting or bracing where necessary.
Other treatment options to further limit the effects of spasticity or reduce early contractures may include medications, progressive casting, surgical correction (i.e., tendon release procedures), motor point blocks, botulinum toxin injections, or an intrathecal baclofen pump. Antispasticity medications exist with various sites of action, ranging from effects at the CNS to effects at the muscle. Patients with early contractures in a monoparesis or hemiparesis pattern may benefit from botulinum toxin injections of involved muscles. Patients with spastic quadriparesis may benefit from placement of an intrathecal baclofen pump. In general, botulinum toxin or intrathecal baclofen may be indicated if reduction of spasticity/early contractures will improve functional independence, hygiene, or comfort or will decrease the risk of skin breakdown.
Prevention of Pneumonia
Pneumonia is a common complication of neurologic illness. Risk factors include depressed cognition, swallowing disorders, and impaired mobility. Risk reduction programs include efforts toward early mobilization as well as prevention of aspiration through modification of diet, alteration of means of nutrition intake if necessary, and proper positioning during feedings. Prolonged bed rest can result in poor aeration of the lungs, atelectasis, and a greater likelihood for development of pneumonia. Early patient mobilization can minimize this risk.
Management of Dysphagia and Aspiration Dysphagia occurs in certain neurologic conditions and may lead to aspiration pneumonia. Swallowing dysfunction can occur as a result of impaired cognition or from incoordination or weakness of the muscles of deglutition. Thus, swallowing is assessed prior to oral feedings in those patients who may be at risk (patients with strokes, brain injuries, neuromuscular diseases, etc.). Signs of possible dysphagia include dysarthria, confusion, frequent coughing, choking on fluids, nasal regurgitation, and pneumonia. Currently, the gold standard of diagnosis is a modified barium swallow study, which can help clarify the phase of swallowing that may be impaired. Goals of dysphagia management include the prevention of aspiration, dehydration, and malnutrition and the restoration of the ability to chew and swallow safely. Treatment includes oral motor exercises, compensatory feeding strategies, modification of food textures, or alternative methods of feeding such as nasogastric tubes or percutaneous endoscopic gastrostomy tubes.
Prevention of Falls, Fractures, and Dislocations
A goal of neurorehabilitation intervention includes ensuring patient safety by preventing falls. The risk of falls is increased in patients with sensorimotor deficits, confusion, or difficulty with communication. Methods to prevent falls vary with the type and severity of the disabilities.
▪ SPECIAL CLINICAL POINT: A fall risk reduction program may include supervision of high-risk patients, toileting at regular intervals, supervision of transfers and ambulation, adapted nurse call systems, and patient and family education.
The use of restraints is avoided whenever possible because restraints may lead to other injuries or cause greater agitation in those already restless.
Another concern is prevention of shoulder dislocations in patients with paretic upper extremities. There is a tendency for subluxation to occur at the shoulder joint capsule as a result of the gravitational pull from the weight of a paretic arm. Preventive measures include maintenance of normal scapulohumeral positioning through physical measures, use of lap trays on wheelchairs, use of pull sheets during bed positioning, and avoidance of excessive range-of-motion exercises. Caution must be taken with lap trays because improper use can lead to nerve injuries or wrist flexion contractures; furthermore, sling arm supports may promote upper-extremity flexion contractures if used improperly. The differential diagnosis for shoulder pain in those with paretic upper extremities also includes rotator cuff tears, adhesive capsulitis, bicipital tendonitis, reflex sympathetic dystrophy, arthritis, and previous injuries.
Prevention in Specific Neurologic Disorders
Patients who have had an ischemic stroke are at substantial risk for a recurrent stroke. Often, the acute-care team will determine the need for carotid endarterectomy or anticoagulation with warfarin, ticlopidine, or aspirin. Neurorehabilitation can help with patient and family education regarding potential modifiable risk factors including hypertension, diabetes mellitus, cigarette smoking, alcohol consumption, drug abuse, obesity, high serum cholesterol, coronary artery disease, left ventricular hypertrophy, and atrial fibrillation.
Spinal cord injuries and disorders can result in a potential for autonomic dysreflexia. This is more likely with high-level cord pathology. Autonomic dysreflexia manifests as precipitous drops or elevations in blood pressure or pulse, often accompanied by a pounding headache, hyperventilation, and flushing or sweating above the level of the lesion. The cause is usually a noxious stimulus involving a numb portion of the body detectable only to the autonomic nervous system. Possible causes may include a full bladder, a fecal impaction, tightfitting clothing or shoes, a skin irritation, a DVT, or an infection. Prevention includes a routine bowel and bladder program, daily skin inspection, and careful dressing. Treatment of acute autonomic dysreflexia includes blood pressure stabilization as well as determination and correction of the etiology.
Autonomic dysfunction also may occur in the setting of acute demyelinating polyneuropathy (Guillain-Barré syndrome). Autonomic symptoms including sinus tachycardia, bradycardia, facial flushing, hypotension, or hypertension; profuse diaphoresis; or even anhydrosis can occur. In addition, urinary retention also may occur in some patients. The autonomic dysfunction associated with acute demyelinating polyneuropathies often remits after a few weeks. Treatment is supportive and expectant.
Early Mobilization and Return to Self-Care
Another goal of acute neurorehabilitation intervention is early patient mobilization and the encouragement of self-care activities.
▪ SPECIAL CLINICAL POINT: Early mobilization helps to prevent DVT, skin breakdowns, pneumonia, joint contractures, and constipation; it promotes early ambulation, better orthostatic tolerance, and performance of basic activities of daily living.
Only gold members can continue reading. Log In or Register to continue