Psychiatry and Residential Care
Stephen W. Brown
Frank M. C. Besag
“Do poor Tom some charity, whom the foul fiend vexes.”
—William Shakespeare, “King Lear,” Act III, Scene IV
“What doubtless remained longer than leprosy, and would persist when the lazar houses had been empty for years, were the values and images attached to the figure of the leper as well as the meaning of his exclusion, the social importance of that insistent and fearful figure which was not driven off without first being inscribed within a sacred circle.”
—Michel Foucault, Madness and Civilization: A History of Insanity in the Age of Reason11
Introduction
Historical Perspective on the Rise and Fall of Confinement
Development of Institutions
Hospitals, hostels, and hotels share functions that are reflected in the common Latin root of these words (hospitalia, “guest chambers”). It is possible that in Europe during the Middle Ages some cities kept hostels for local people who were not capable of looking after themselves. Also, some people with behavioral problems that would now be attributed to psychosis, brain damage, or other psychiatric conditions might congregate around certain religious shrines. Custodial institutions that were separate from prisons appeared in Europe from the late 17th century onward and, during the 18th century, there emerged specialized asylums for the insane. The reason for the growth in asylum building during that period of history has been a subject of speculation in this century. One argument has been that a real increase occurred in the population with psychosis.12 Alternatively, sociologic explanations have been advanced, suggesting that the development of psychiatry was a self-perpetuating means of social control.25 For example, Foucault, noting that leprosy had recently disappeared from Europe, postulated that the “formulas of exclusion” persisted, so that “…poor vagabonds, criminals, and ‘deranged minds’ would take the part played by the leper …,” and he refers to “…that major form of a rigorous division which is social exclusion but spiritual reintegration.”11 Houses of correction were established in England in 1575 by an act of Parliament for “the punishment of vagabonds and the relief of the poor,” and in 1656 the Hôpital Général was founded in Paris to confine the poor. Foucault notes that this confinement included “the debauched, spendthrift fathers, prodigal sons, blasphemers, men who ‘seek to undo themselves,’ libertines, and, in about one-tenth of cases (Paris), the insane.” There was, however, a gradual process of categorization whereby those in need of asylum were recognized as being respectively poor, insane, handicapped, or epileptic, and these groups in turn came to be regarded as separate from criminals. As asylums increased in number and became more concerned with mental illness, a more humane approach to care appeared. This was typified by the work of William Tuke (1732–1822) in York (who founded the York Retreat after the death of a fellow Quaker in the county asylum), and Philippe Pinel (1745–1826) in France. Both stressed moral aspects of treatment and advocated the avoidance of methods of physical constraint, such as chains. Pinel’s pupil Maisonneuve studied epilepsy, and wrote that “…epilepsy, like all chronic diseases, can be studied well only in the hospitals; there alone is it possible to find all its varieties together, to see all its nuances, and to acquire in short time more experience of this disease than in the whole course of ordinary practice.”16 Another physician of Maisonneuve’s generation, Jean Etienne Dominique Esquirol (1772–1840), advocated special facilities for people with epilepsy apart from the other asylum inmates. The reason for this, however, was not to protect those with epilepsy, but to protect the insane, for he believed “…that the sight of one epileptic attack might suffice to make a healthy person epileptic. Now if this held true of healthy people, how much greater was the danger for the mentally deranged, who were so much more impressionable.”27 Consequently, with the growth of provision for the insane there also came separate facilities within the asylums for people with epilepsy. It is not surprising that the next stage was the establishment of entirely separate institutions for people with epilepsy.
Epilepsy in Institutions and the Move Toward Colonies, Villages, and Schools
European writers of the 19th century became interested in the ways in which epilepsy might act on the mind and cause mental disorder. Morel23 suggested that the disease could exist in a masked form (epilepsie larvée), in which the main features were of insanity, not seizures. Falret10 attempted to classify the psychiatric disorders of epilepsy and, in addition to acknowledging the existence of interictal and peri-ictal phenomena, he followed Morel in proposing a category of epileptic insanity that was manifested as an alternative to seizures, the folie épileptique. Morel also offered the view that the behavioral disorders associated with epilepsy, in particular the “epileptic furore,” might be a consequence of bad treatment, and that improvement of the patient’s environment by segregation, recreation, and occupation would bring about improvement.22 This debate added to the intellectual climate from which the argument for separate institutions for epilepsy was to emerge.
In 19th century Europe, the word colony did not carry a pejorative connotation. The notion of establishing separate living space for people with epilepsy was based on a belief that this would be therapeutic in itself. There was an understanding that the condition was perpetuated by restrictions placed on the activities of normal life, especially the opportunity to take part in work. This was the rationale for the colony movement,
exemplified by the foundation in 1867 of Bethel, near Bielefeld in Germany, and by the foundation later in England of the Chalfont, Lingfield, and David Lewis colonies, and in the United States of the Craig colony. The emphasis was on social management, with early intervention by admission to the colony; discharge back to society was a possibility. Alan McDougall, the first medical director of the David Lewis colony, wrote, “Most of our colonists come to us too late to be cured of their fits. The children give brilliant results; one third of them become free from fits. Our… experience seems to show that if all epileptic children, whatever their social position, were sent on the first appearance of epileptic symptoms to an epileptic colony, and kept there till the end of their school life, the benefits to themselves, to their relatives, and to the State would be enormous.”19 These epileptic colonies were sometimes, but not exclusively, situated in the countryside. They typically created a village-like atmosphere, and often included a residential school for children with epilepsy. Attention to lifestyle, as well as physical treatment, was considered important: “Most of the colonists take daily a 30-grain dose of Potassium Bromide. This appears in many cases to diminish the frequency of the fits, and the tendency to status. But other therapeutic means are even more important. Among these is the combined concert and dance that has been held without intermission every Saturday night of the year. Dancing (particularly the ‘Lancers’) is a valuable means of treatment, provided that it be practised frequently. On the first few occasions a fit may follow the dancing, but the patient soon becomes able to dance without unpleasant side effects. Classical treatment of Epilepsy follows the lines of forbidding the patient to do the things that might cause a fit; colony treatment attempts to rid the patient of fits while he is performing the acts of a normal person. The latter plan gives the better results.”17
exemplified by the foundation in 1867 of Bethel, near Bielefeld in Germany, and by the foundation later in England of the Chalfont, Lingfield, and David Lewis colonies, and in the United States of the Craig colony. The emphasis was on social management, with early intervention by admission to the colony; discharge back to society was a possibility. Alan McDougall, the first medical director of the David Lewis colony, wrote, “Most of our colonists come to us too late to be cured of their fits. The children give brilliant results; one third of them become free from fits. Our… experience seems to show that if all epileptic children, whatever their social position, were sent on the first appearance of epileptic symptoms to an epileptic colony, and kept there till the end of their school life, the benefits to themselves, to their relatives, and to the State would be enormous.”19 These epileptic colonies were sometimes, but not exclusively, situated in the countryside. They typically created a village-like atmosphere, and often included a residential school for children with epilepsy. Attention to lifestyle, as well as physical treatment, was considered important: “Most of the colonists take daily a 30-grain dose of Potassium Bromide. This appears in many cases to diminish the frequency of the fits, and the tendency to status. But other therapeutic means are even more important. Among these is the combined concert and dance that has been held without intermission every Saturday night of the year. Dancing (particularly the ‘Lancers’) is a valuable means of treatment, provided that it be practised frequently. On the first few occasions a fit may follow the dancing, but the patient soon becomes able to dance without unpleasant side effects. Classical treatment of Epilepsy follows the lines of forbidding the patient to do the things that might cause a fit; colony treatment attempts to rid the patient of fits while he is performing the acts of a normal person. The latter plan gives the better results.”17
The development of colonies was the consequence of a philanthropic movement spearheaded by the social and religious conscience of the aristocracy and upper middle classes. Increasingly, the new wealthy class—the industrial bourgeoisie—undertook a scheme of building model villages for the working classes, exemplified by the work of the Cadburys in Bournville in the English Midlands, and in the building of Styal Village for the workers of Styal Mill in Cheshire. Also at this time, arts and crafts colonies developed, where a particular creative lifestyle could be followed, away from a society that Crichton-Browne described as “…a feverish and fidgety age in which an unappeasable restlessness pervades all ranks and classes.”7 This movement was not in any way the consequence of an overt desire to segregate or discriminate against elements of society regarded as difficult, dangerous, or undesirable. Thus, at this point, the history of the institutional management of epilepsy should diverge from that of institutional psychiatry. In particular, the epilepsy colonies (in Europe at least) were concerned from the beginning with destigmatization and normalization, with attaching value to people’s social roles. The evidence is in stark contrast to that often offered by historians as explanations for the great confinement of the mentally ill in the 17th, 18th, and 19th centuries. Why is this? One explanation might be that some of the accepted historical cases in psychiatry have been overstated. Bynum wrote of Foucault, “…the power of his dark vision remains, although its empirical base has been questioned,”3 and another modern historian noted, “…the view that the 17th and particularly the 18th centuries were a disaster for the insane in England has to be qualified….”24 Alternatively, perhaps the epilepsy colony movement then was in opposition to social attitudes at the time. Indeed, the views of those advocating colony treatment are not congruent with ideas expressed by eminent psychiatrists much later in the 20th century. For example, in 1977, a leading English-language textbook of psychiatry contained the following passage describing personality deterioration in epilepsy: “There are also more constant and lasting affective changes. Most frequently these take the form of a mulish moroseness and rancour. Slights are felt to the quick, and malice is borne for months or years. In an epileptic ward gossip, lying or slander will all too easily reign…. Chronic epileptic patients are capable of actions of the most malicious and petty spite, and of combining them with self-justification and self-praise.”26
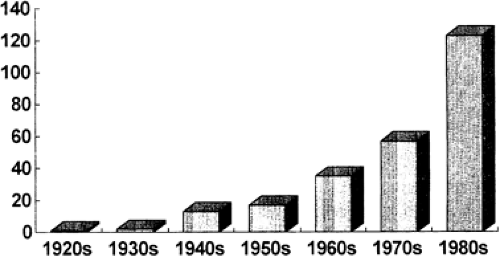 FIGURE 1. Admission rates to the Davis Lewis Centre for Epilepsy, 1920–1989. |
Seven decades earlier, in 1909, Alan McDougall had noticed the opposite: “Each succeeding year, in spite of the constant increase in the population, there is less and less quarrelling among the colonists. Our experience leads us to believe that many of the unpleasant characteristics commonly ascribed to epileptics are due not so much to the disease as to the mishandling that the patient has received. When living with those who understand his special requirements, the epileptic is a very likeable person.”19 McDougall, however, did have a sanction that was not available to the alienist and, in the 1906 colony report, he noted, “Four have been discharged as unsuitable. Their persisting lack of consideration for their fellow colonists made it impossible to retain them. Yet had they entered a colony at an early stage of their illness, they would probably have been excellent colonists.”17
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


