53 Spinal Cord Tumors
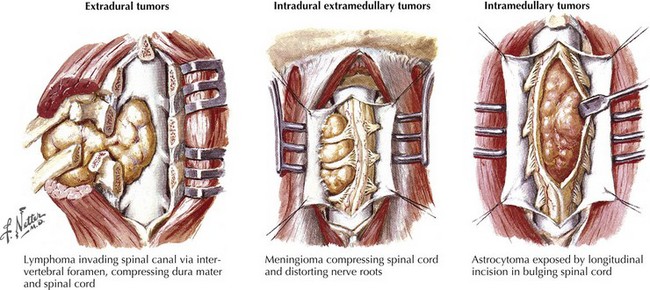
The most common spinal cord tumors are metastatic extradural lesions usually but not always occurring in patients with already identified malignancies, either cancers or lymphomas. Their presentation is often relatively acute, usually associated with focal back and/or radicular pain. On occasion, these lesions are the initial clinical manifestation of a heretofore unsuspected systemic malignancy. In contrast, primary intradural spinal cord tumors occur infrequently; typically their presentation is a relatively subtle one, ingravescent in temporal profile. Spinal cord and spinal column tumors are best classified within two categories: extradural, occurring outside of the dura, and intradural, contained within the dura mater (Table 53-1; Fig. 53-1).
Table 53-1 Classification of MRI Abnormalities*
| Extradural Extramedullary | Intradural Extramedullary | Intradural Intramedullary |
|---|---|---|
| Disc disease | Neurinoma | Syringomyelia |
| Metastatic carcinoma | Meningioma | Tumor |
| Lymphoma | Intracranial tumor seeding | Ependymoma |
| Sarcoma | Ependymoma | Glioma |
| Plasmacytoma | Medulloblastoma | Hemangioblastoma |
| Primary bone tumor | Glioma | Myelitis |
| Scar | Cauda equina lesions | Edema |
| Abscess | Scarring | Lipoma |
| Hemangioma | Hypertrophic neuropathy | Rare lesions |
| Rare lesions | Rare lesions | Abscess |
| Hemorrhage | Lymphoma | Hematoma |
| Neurilemmoma | Metastasis | Varix with AVM |
| Meningioma | Hemangioblastoma | Lymphoma |
| Chordoma | Lipoma | Neuroblastoma |
| Dermoid | Metastasis | |
| Epidermoid | ||
| Cyst | ||
| Clot |
* Dermoid or epidermoid, teratoma, lipoma, and cysts are often associated with spinal dysraphism. In this setting, many tumors are intradural, although they may involve all three areas.
Extradural Spinal Tumors
Clinical Vignette
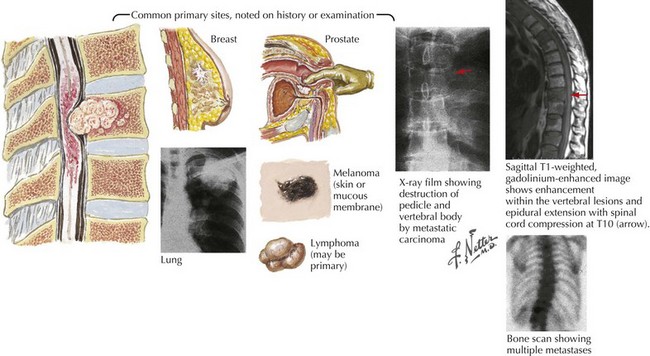
Spinal radiographs revealed destruction of the T9 vertebral body. Magnetic resonance imaging (MRI) demonstrated a soft tissue mass involving most of the T9 vertebral body, extending into the pedicle, with epidural extension of the tumor into the spinal canal leading to marked compression of the spinal cord. Immediate dexamethasone and subsequent radiation therapy was unsuccessful in reversing his clinical course. Chest radiograph (Fig. 53-2) demonstrated a left main stem bronchus tumor that on biopsy proved to be a primary small cell lung cancer.
Clinical Presentation
Severe focal vertebral pain is frequently the presenting symptom of a metastatic spinal cancer (Fig. 53-2). Unfortunately, back pain is such a ubiquitous complaint that the serious nature of a newly occurring pain is often not appreciated even when there is no history of recent trauma. Sometimes, it is difficult to distinguish pain of a metastatic spinal tumor from the much more common mechanical, degenerative, or osteoarthritic musculoskeletal lower back and/or nerve root disorders. However, pain of metastatic spinal cancer origin is often persistent, frequently unrelated to posture, and tends to increase at night. In contrast to more common mechanical back pain, this pain can be of more recent origin.
Typically, the course of extradural metastatic spinal tumors is more rapid than intradural tumors. It is not unusual for these lesions to have an almost precipitous onset, often producing rapidly evolving motor and sensory deficits within just a few hours to a day or so (Fig. 53-3). A prior diagnosis of either a cancer or a lymphoma will alert the astute clinician to the precise pathophysiologic nature of the spinal lesion. However, occasionally a spinal metastasis may be the initial presentation of a metastatic malignancy.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


