Figure 90.1. Magnetic resonance imaging with multiple lesions hyperintensitive in diffusion-weighted, sequences.
Angiography is useful in the detection of lesions in medium and large vessels. However, when smaller sized branches are affected, and generally with distal compromise of the middle cerebral artery, digital angiography is the method of choice, with a sensitivity and specificity of 50% for the detection of characteristic lesions in the shape of rosary beads (Figure 90.2).
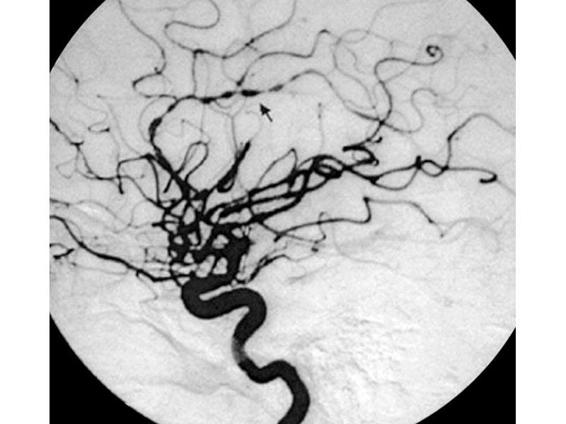
Figure 90.2. Digital angiography with lesions in the shape of rosary beads (arrow).
In systemic vasculitis with repercussions in the CNS, the involvement of different organs generally allows for diagnosis, while in primary vasculitis of the CNS cerebral biopsy and leptomeninges are considered the gold standard by most authors. The lack of clinical signs with the high specificity and low efficiency of complementary studies would require a cerebral biopsy when a diagnosis of primary vasculitis of the CNS is suspected.
In a study by Alrawi et al. only 36% of patients suspected with vasculitis of the CNS were anatomopathogically confirmed, while the remaining 64% had either another disease or the biopsy was not diagnostic. Two patterns have been described in vasculitis: necrotizing granulomatosis in large vessels and nongranulomatous lymphocytic vasculitis of the small vessels (Figure 90.3).
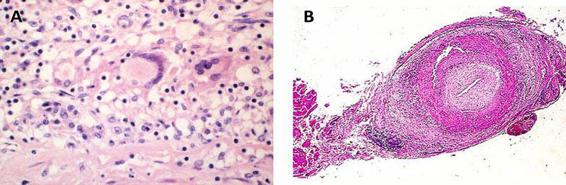
Figure 90.3. Two different patterns of vasculitis: necrotizing granulomatsis in large vessels and nongranulomatosis lymphocitic vasculitis of the small vessels.
90.4 Pathogenesis
Different immunological mechanisms that are not mutually exclusive are involved in the pathogenesis of the inflammation and damage of the vascular wall. The most common is caused by the formation of immune complexes, as in serum disease. Attachment of immunocomplexes to the vascular wall induces adherence and activation of the complement cascade, with immune amplification through the release of cytokines, the consequent expression of adhesion molecules in their membranes, and the release of their lysosomal products, with damage to the endothelium and other components of the vascular wall. Other mechanisms involved in vascular damage include: anticellular endothelial and antilysosomal antibodies and the creation of a cellular type of immune response with the formation of granulomas.
90.5 Differential Diagnosis
It is worth noting here that there are illnesses that are not classically considered as vasculitis but that share anatomopathological features with it, such as:
- Severe hemorrhagic encephalomyelitis with perivenular inflammatory infiltrates, such as in demyelinating diseases and vascular wall necrosis.
- Reversible posterior leukoencephalopathy where there is an opening of the narrow endothelial unions due to toxic or secondary hemodynamic changes.
- Inflammatory changes in atherothrombotic disease.
The main differential diagnoses of vasculitis of the CNS are summarized in Table 90.4. Figure 90.4. reports a flow-chart for the management of these patients.







