Suprasellar Mass, General
Anne G. Osborn, MD, FACR
DIFFERENTIAL DIAGNOSIS
Common
Pituitary Macroadenoma
Meningioma
Saccular Aneurysm
Craniopharyngioma
Pilocytic Astrocytoma
Less Common
Dilated Third Ventricle
Arachnoid Cyst
Neurocysticercosis
Rathke Cleft Cyst
Neurosarcoid
Langerhans Cell Histiocytosis
Germinoma
Dermoid Cyst
Lipoma
Rare but Important
Lymphocytic Hypophysitis
Tuber Cinereum Hamartoma
Epidermoid Cyst
Pituicytoma
Diffuse Astrocytoma, Low Grade
Pilomyxoid Astrocytoma
Ectopic Neurohypophysis
Metastasis
Lymphoma, Metastatic
Leukemia
Cavernous Malformation
Tuberculoma
Pituitary Abscess
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Is mass arising from pituitary or other site?
Does it mostly involve infundibular stalk?
Is patient adult or child?
Helpful Clues for Common Diagnoses
Most common diagnoses (“big five”) account for > 75% of all suprasellar masses
Pituitary Macroadenoma
Most common of all suprasellar masses = suprasellar extension of macroadenoma
Gland, mass can’t be separated
Cystic, hemorrhagic changes common
Mass is the pituitary gland
Meningioma
Arises from diaphragma sellae
Thin black line (diaphragma sellae) separates mass from pituitary
“Dural tail sign”
Not pathognomonic but highly suggestive
Signal intensity following contrast usually > tumor itself
Saccular Aneurysm
Most arise from circle of Willis
Are usually slightly eccentric, not midline
Signal intensity may be mixed
Partial/complete thrombosis common
Complex/disturbed flow may cause spin dephasing
Look for phase artifact
Occasionally fusiform aneurysm/ectasia of basilar artery may project into suprasellar cistern
Craniopharyngioma
Most common suprasellar mass in child
Adamantinomatous subtype
Imaging
90% Ca++, 90% cystic
90% enhance (rim ± nodule)
Second peak in middle-aged adults
Papillary subtype
Solid > cystic; Ca++ uncommon
Pilocytic Astrocytoma
Second most common suprasellar mass in children (rare in adults)
Hypothalamus/optic pathways
Pilocytic > > pilomyxoid type (see below)
Helpful Clues for Less Common Diagnoses
Dilated Third Ventricle
Most common “cystic” suprasellar mass
Third ventricle enlarged secondary to obstructive hydrocephalus
Arachnoid Cyst
Elevates, displaces third ventricle
Neurocysticercosis
Suprasellar cistern, sylvian fissures common sites
Variable size cysts, enhancement
Reactive meningeal changes may be striking (e.g., stalk thickening, vascular encasement)
Rathke Cleft Cyst
Look for intracystic nodule
Pituitary displaced by mass
Neurosarcoid
Langerhans Cell Histiocytosis
Thickened stalk, child with DI
Germinoma
Stalk ± gland
Can be only site but look for pineal mass
Dermoid Cyst
Fat-like ± droplets (ruptured)
Lipoma
Fatty mass stuck on hypothalamus
Use fat-saturated T1WI
Helpful Clues for Rare Diagnoses
Lymphocytic Hypophysitis
Thick, nontapering stalk ± pituitary mass
Diabetes insipidus common
Often occurs in peripartum females
Tuber Cinereum Hamartoma
Clinical presentation helpful (gelastic seizures; male with precocious puberty)
Can be “collar button” or “sessile”
Between infundibulum (anteriorly), mammillary bodies (posteriorly)
Signal intensity like cortex
Does not enhance
Pituicytoma
Low grade (WHO I) glial neoplasm of infundibulum or neurohypophysis
M > F, most patients 40-60 years
Hypopituitarism, visual disturbances
Well-demarcated, homogeneously enhancing infundibular mass
Diffuse Astrocytoma, Low Grade
Infiltrating mass difficult to distinguish from pilocytic astrocytoma (PA)
Pilomyxoid Astrocytoma
Rare, more aggressive PA variant
Infant/young child with bulky H-shaped suprasellar mass
Often hemorrhages (PA, low grade do not)
Metastasis
Gland ± stalk mass in patient with known primary
Lymphoma, Metastatic
Destructive, infiltrative mass engulfs gland, stalk
Leukemia
Gland/stalk + sinus mass clues
Cavernous Malformation
“Popcorn ball” mass
Third ventricle, optic chiasm rare sites
Tuberculoma
TB meningitis > > frank tuberculoma in suprasellar cistern
Focal mass w/ring enhancement common
If caseating, mass is hypointense on T2WI
If noncaseating, mass generally hyperintense on T2WI
Pituitary Abscess
Very rare but potentially life-threatening
May resemble pituitary apoplexy at imaging
Cystic-appearing intrasellar mass with suprasellar extension
Hypodense on NECT
Hyperintense on T2WI
Rim-enhancing
Image Gallery
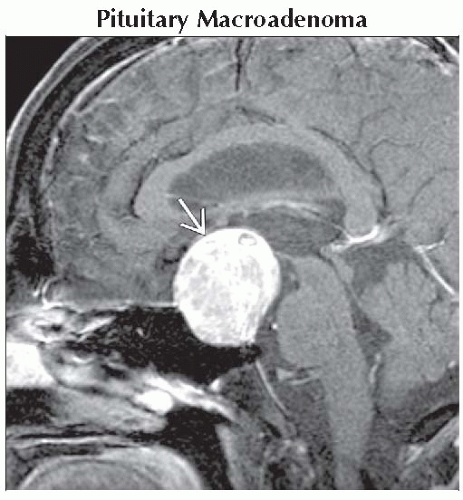 Sagittal T1 C+ FS MR shows a pituitary macroadenoma  . The pituitary gland cannot be seen separate from the mass. The mass is the gland, which is diffusely enlarged by the tumor. . The pituitary gland cannot be seen separate from the mass. The mass is the gland, which is diffusely enlarged by the tumor. |
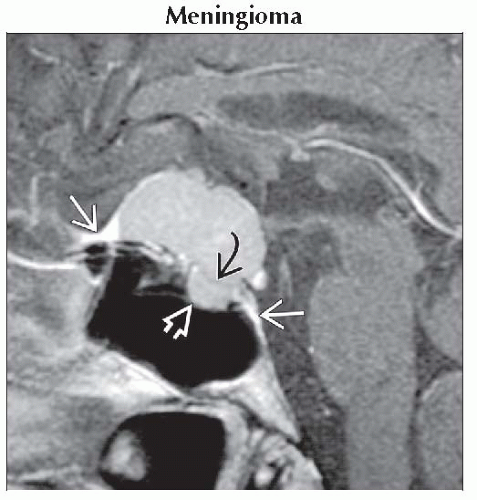 Sagittal T1 C+ MR shows a classic suprasellar meningioma arising from the diaphragma sellae  , which clearly separates the mass from the normal pituitary below , which clearly separates the mass from the normal pituitary below  . Note dural “tails” . Note dural “tails”  . . |
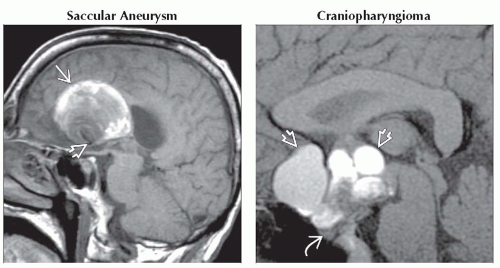 (Left) Sagittal T1WI MR shows a large, mixed signal intensity, suprasellar mass
 . Laminated clot of different ages gives mass an “onion skin” appearance. Note residual patent lumen . Laminated clot of different ages gives mass an “onion skin” appearance. Note residual patent lumen  . (Right) Sagittal T1WI MR shows a craniopharyngioma . (Right) Sagittal T1WI MR shows a craniopharyngioma  with variable T1 shortening within the multiloculated cystic components. The pituitary gland with variable T1 shortening within the multiloculated cystic components. The pituitary gland  is clearly distinct from the mass. is clearly distinct from the mass.Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|