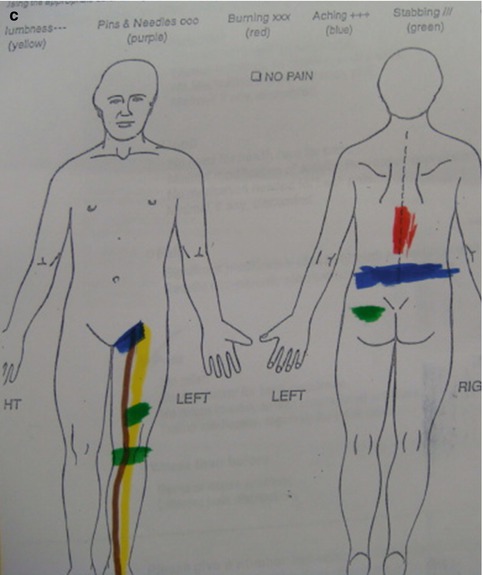
Fig. 6.1
(a) Typical adult degenerative scoliosis demonstrating the major curve in the mid-lumbar spine with a compensatory fractional curve at the lumbosacral junction. (b) Also note the loss of normal lordosis at the lumbosacral junction. (c) The patient’s preoperative pain drawing showing symptoms of an L5 radiculopathy due to foraminal stenosis associated with the fractional curve
6.2 Biomechanics of the Fractional Curve
Surgeons treating scoliosis should pay special attention to the lumbosacral junction. In traditional open surgery, fusions will often involve the lumbosacral junction, and successful operations need not pay special attention to this area as an open exposure will allow for neural decompression, fusion, instrumentation, and segmental manipulation to correct any local deformity. For example, due to difficulties in achieving an L5–S1 fusion, many surgeons will perform an adjunct anterior lumbar interbody fusion. While this approach adds the risks and morbidity of a second surgical approach, it offers several distinct advantages: (1) The ample exposure of the disc space unencumbered by neural elements allows the surgeon to place a graft with a large surface area for fusion. (2) The ability to place this large interbody spacer or graft improves anterior load sharing, off-loading stress from the posterior fixation hardware. (3) Distraction of the disc space also opens the neural foramen, indirectly decompressing the neural elements. (4) Removal of the anterior longitudinal ligament allows for application of significant forces to distract the disc space. This affords the opportunity to add up to 15° degrees of lordosis to the spine. (5) Improving sagittal and coronal alignment at the lumbosacral junction translates into greater effects up the spinal column than an equal correction in the mid-lumbar spine. In essence, then, the addition of a L5–S1 or L4–S1 ALIF will effectively deal with any fractional curve issues. Other methods for handling the fractional curve in open surgery include PLIF or TLIF, posterior decompression, and segmental manipulation of the screws and rods to achieve deformity correction.
In a review by McPhee and Swanson, correction of the fractional curve via a staged procedure resulted in a substantial correction of scoliosis, lordosis maintenance, and high arthrodesis rates. Furthermore, these radiographic findings were correlated with a greater more improvement in function than with posterior surgery alone [1]. Given these factors, both traditional and MIS surgeons should pay special attention to the fractional curve. Preoperatively, an assessment of the fractional curve’s role in compensating for the major curve, its degree of flexibility, the amount of sagittal correction needed in this area, and any local neural element compression in this area is all critical in preoperative planning. Preoperative MRI, lateral bending X-rays, and 36 in. standing films can be helpful for preoperative patient evaluation.
6.3 Neural Entrapment at the Fractional Curve
In a study by Fu et al. of 36 patients with adult scoliosis, at least one level of severe foraminal stenosis was identified in 97 % of patients, and all but one of these patients had significant radicular pain. 19 % of patients presented with multiple levels of symptomatic nerve root entrapment, 76 % had pain corresponding to areas of the most severe foraminal stenosis, and 24 % had pain corresponding to areas of moderate stenosis [2]. During the preoperative evaluation, it is critical to identify the symptomatic level(s) of nerve entrapment, if there is concomitant leg pain. Fractional curve radiculopathies will typically involve L5 or S1, thus radiating down the posterior thigh and into the dorsum or sole of the foot (Fig. 6.1). Pain that is more localized to the anterior thigh or groin is typical of mid- and upper-lumbar radiculopathy and thus associated with the major curve.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


