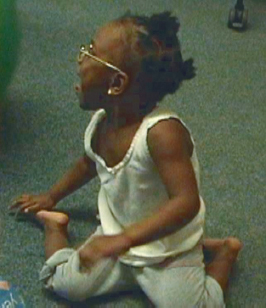
17 The Practice of Physical Therapy from a Neuro-Developmental Treatment Perspective This chapter first traces the history of the profession of physical therapy (physiotherapy), which provides the reader with a focus that continues to influence the profession today. The addition of the Neuro-Developmental Treatment (NDT) Practice Model and its influences on the profession follow, along with specific examples of problem solving and decision making using commonly addressed activities and participation that physical therapists (PTs) encounter. Learning Objectives Upon completing this chapter the reader will be able to do the following: • Define who a physical therapist/physiotherapist (PT) is in terms of professional responsibilities and functional outcomes addressed in client management. • List at least three skills NDT education enhances in the professional skills of PTs. • Analyze a physical therapy outcome with a specific participation or activity of a client in the reader’s own practice using the NDT Practice Model. Physical therapists or physiotherapists (PTs) “are health care professionals who diagnose and treat individuals of all ages, from newborns to the very oldest, who have medical problems or other health-related conditions that limit their abilities to move and perform functional activities in their daily lives.”1 Physical therapy as a profession provides clinical services aimed at the acquisition, refinement, restoration, maintenance, and rehabilitation of physical function.2 These services include diagnosis and management of movement dysfunction and the promotion of physical wellness, fitness, and prevention of injury and disability. PTs manage their patients or clients through a process of examination, evaluation, diagnosis, prognosis, and intervention using therapeutic measures to achieve functional physical outcomes. They manage their patients and clients to alleviate pain; prevent onset or progression of impairment, activity limitation, and participation restrictions due to injury or disease; and restore, maintain, and promote overall fitness, health, and optimal quality of life.3 Although the profession has always been closely aligned to the medical profession, current entry-level education and licensure in many countries or parts of countries allow autonomous practice. The official origin of the practice of physiotherapy can be traced back to Per Henrik Ling in 1813 with the founding of the Royal Central Institute of Gymnastics. Ling is known as the father of Swedish Gymnastics. The Institute was founded for massage, manipulation, and exercise. Through Ling’s experiences in England, Germany, and France, and with a Chinese man who taught him martial arts, he realized the importance of using exercises for the health of others.4 The roots of the physical therapy profession may have begun much earlier, however, with evidence for the practice of massage in China as early as 3000 BC. There are also references to friction massage from Hippocrates (460–377 BC).5 History and oral stories in many cultures describe hands-on physical manipulation in medical treatment, exercise for health benefits, hydrotherapy, protocols for individuals postparalysis and paresis, and therapeutic massage dating before the Common Era.5,6,7,8 Thus the use of physical therapy to heal and rehabilitate was developed over thousands of years.9 In the late 19th century/early 20th century, two major historical events occurred that caused a fundamental adjustment to the practice of physical therapy.9,10 Healing and restoration of physical function after traumatic injury during combat during World War I created a cohesive structure for a group of women called reconstruction aides. In the United States, this group of women with physical education backgrounds completed courses in anatomy and physiology and in care of individuals postamputation, postfracture, and with nervous disorders prior to being sent internationally to hospitals.10 The second group of individuals requiring this group’s services resulted from poliomyelitis epidemics.11 The intense attention to rehabilitation of the respiratory and neuromusculoskeletal systems in individuals with polio eventually broadened to the care of individuals with other pulmonary problems and to those who had had a stroke or who had cerebral palsy (CP).11 As physical therapy broadened from serving wounded soldiers and those with polio to a variety of individuals seeking physical habilitation and rehabilitation, educators, clinicians, and researchers began to develop an interest in various patient populations. The unique posture and movement impairments of individuals poststroke and those with CP, as well as the functional outcome needs of these two groups of people, drove the profession to learn more about each condition. As a result, PTs began a more focused look at two areas of physical function: development of motor skills and recovery of motor skills after a brain injury. In the 1940s and 1950s, a dissatisfaction with the sole use of the orthopedic approach to surgery and bracing as a model for rehabilitation for these two groups led therapists to study how the central nervous system (CNS) works to more effectively treat individuals poststroke and with CP.12 According to historical summaries by Gordon12 and Cohen and Reed,13 neurophysiological (or neurotherapeutic) approaches resulted and evolved: among these approaches were those of Kabat and Knott (proprioceptive neuromuscular facilitation), Rood, Brunnstrom, and Bobath and Bobath. All neurophysiological approaches, including the Bobath approach that the Bobaths later named Neuro-Developmental Treatment (NDT), continue to evolve according to clinical observations and intervention results as well as the continual knowledge gained in the basic sciences. As noted in the brief history of physical therapy, the profession began as a medically oriented one, with an emphasis on anatomy and physiology. Worldwide, physical therapy education is now recommended to include the study of the anatomy and physiology of all body systems, biomechanics and kinesiology, exercise physiology (including posture and movement), and exercise prescription.14 Entry-level education for PTs in many countries has a long tradition of single- and multisystem posture and movement analysis, including effective, ineffective, and compensatory posture and movement analysis. Physical therapy and physical therapist assistant (PTA) education focuses on biomechanical principles of human motion throughout anatomy and kinesiology courses. The PT brings all of this specialization to the NDT Practice Model as the movement analysis expert on the health care team. The PT has in-depth knowledge of neuromusculoskeletal anatomy and physiology and a strong background in analyzing body systems in terms of mechanical stability and instability, synergistic action of muscles, and neuromusculoskeletal health and disease/disability. Posture and movement are familiar terms in physical therapy. Entry-level education prepares the PT and PTAs (in countries that educate PTAs) with postsecondary education to assess integrities and impairments in many body systems, including neuromuscular, musculoskeletal, respiratory, and sensory systems’ reception and processing. From the roots of the profession in massage, manual techniques, and exercise, to the more recent evolution of the specialized practice of manual therapy, physical therapy has long been considered the discipline within the health care team to provide the expertise in manual handling skills. The PT brings this skill to the practice of NDT where handling is one of the hallmarks. In today’s professional practice, PTs combine the centuries-long knowledge and skill base in the use of manual therapy and exercise, with the evidence supporting the potential for recovery of damaged neural tissue, to work with individuals who have dysfunctions of the CNS. The NDT Practice Model further adds to this skill set by honing the PT’s understanding and integration of the role of the body’s posture and movement systems in producing efficient movement that enables the individual to function at the level of the Activity and Participation domains of the International Classification of Functioning, Disability and Health (ICF). NDT broadens the application of entry-level education for PTs into a structured practice model where the PT applies knowledge to the following: • A focus on individualized, specific functional outcomes. • Detailed biomechanical and kinesiological analysis of past, present, and potential future postures and movements. • Intervention that affects whole-body function, posture, and movement. • A big picture view of the effects of current function, posture, and movement on future function and body systems. Bobath15 stated in 1977, “[The therapist] must have a thorough knowledge of normal co-ordination and of the most essential ‘basic patterns’ which underlie a skill and make it possible. Only then can a systematic preparation for functional skills be made.” In this same article, Bobath15 advises therapists who are working with clients poststroke to note changes in postural tone and coordination of posture and movement, loss of normal movement patterns, loss of sensation, and loss of strength. She analyzed body system structures and functions long before the profession of PT as a whole began to do so. Bobath’s handling of her adult and pediatric clients was always taught as a means of assessment as well as treatment. She taught that handling could be used as assistance for body segment support, guidance and assistance of posture and movement, and sensory input. She taught that handling should be systematically withdrawn as the client is able to control and coordinate posture and movement.16 She gave to the physical therapy profession the ability to observe constantly throughout intervention and to respond to the client constantly. She insisted that PTs observe and treat the entire body. She taught PTs that they could change the outcomes for people poststroke and people with CP.17 So much of this mindset seems a part of standard PT practice now, but we may not know how it originated. The core curriculum in current NDT education includes careful observation and handling to assess the posture and movement strategies of each client to determine whether they are functionally effective or ineffective. This analysis includes predictions of future postures and movements based on the current repertoire of the client. Effective postures and movements expand the client’s functional possibilities. Ineffective and compensatory postures and movements are thoughtfully analyzed and weighed as to their potential both to allow current function and to assist or impede future functioning. They are not accepted as inevitable nor are they viewed as completely unacceptable in and of themselves. In NDT education, ineffective and compensatory postures and movements are explored as to their potential to assist with function and to limit function. The ICF model assists in an understanding of the influence of ineffective and compensatory postures and movements on current and future activity and participation. The PT uses this information to become a more expert practitioner, who applies the depth of constant observation, the constant response of the client, detailed analysis of posture and movement, and whole-body and life span viewpoints to continue education beyond entry-level education. An example of using the NDT Practice Model as a PT illustrates how NDT education deepens the PT’s problem-solving skills. A child with CP often uses W-sitting as a functional way to sit on the floor (Fig. 17.1). This sitting posture allows balance and control of sitting in the presence of restricted hip mobility (especially hip abduction and external rotation range) and limited muscle length (especially length of the hip flexors, medial hamstrings, and hip adductors). W-sitting provides the child with a large base of support within these ranges of motion and muscle length impairments, providing structural stability to the child’s trunk, which also may be limited in antigravity control and mobility. The position of the hips in flexion, internal rotation, and varying ranges of abduction/adduction, along with the trunk positioned between the hips in a way that limits the necessity of full sagittal, frontal, and transverse plane control for an upright position, provides skeletal stability to free the child’s arms for play. This play, of course, is the functional desire of the child, who is unconcerned with how posture and movement must be achieved. A physical therapist and parent are concerned about how the child sits, however, for several reasons. • The posture, if practiced for prolonged periods, does not promote joint mobility and muscle length changes, especially in the trunk and lower extremities. It is ineffective in expanding neuromuscular, musculoskeletal, and perceptual functions as well as preventing the development of more effective postural control necessary for a variety of activities and participation. Fig. 17.1 This child with spastic cerebral palsy W-sits. This position allows her to use her arms for play in the presence of posture and movement impairments in her lower body. • Spinal and lower extremity (LE) positions used in W-sitting may predominate in other positions, most notably standing and walking, which contributes to high energy cost and potential joint damage. Therefore, limited choices for body segment alignment and muscle activity interfere with all activities now, not just sitting choices. • High energy cost, joint damage over time, and limited opportunities for more complex postures and movements to develop may result, thereby limiting functions such as community-level ambulation, running, and stair climbing, as well as participation using these activities. The NDT-educated PT understands, however, that the solution is not simple and easy. Simply telling the child and family that the child is not allowed to sit that way because problems could result leaves the child with no alternatives for function. The PT knows that if she recommends that a child no longer use W-sitting in spontaneous, functional floor play, a solution to floor sitting that is just as easy to get in and out of and that allows use of the arms for play is necessary for the recommendation to be easily accepted. Unfortunately, such a solution is rarely readily available. The PT must weigh many considerations when offering potential alternatives to W-sitting for floor play. They include, but are not limited to, the following: • How easy will it be for the child to get in and out of an alternate sitting position? • Will the alternative allow the child to play as easily and safely as when she is W-sitting? • Will an alternative solution potentially cause another set of posture and movement and therefore function problems? The PT, family, and possibly the child herself must discuss and problem-solve about this situation in a way that embraces the unique functioning of the family. Can the child be seated at a table or in a booster chair for play sometimes (this requires adult assistance) in a way that will promote erect postural control in the trunk and weight shifting from one hip to the other? Can the PT incorporate posture and movement intervention strategies into the current plan of care to accomplish alternative sitting positions that the child can effectively assume and sustain spontaneously or with some level of parental assistance? What may be the long-term participation restrictions if the child cannot achieve another floor-sitting position? Are these restrictions significant enough that measures to eliminate floor sitting from the child’s repertoire of play are deemed necessary even when the child may not readily accept this solution? Adults poststroke often begin to live and function on the less involved side of their body. They learn to sit, transition between postures, stand and walk, all with a heavy dependence on the less involved arm and leg. Therapy approaches may direct the individual to strengthen these strategies with repeated practice of functional tasks that emphasize the reliance on the less involved limbs. These strategies may include transfer practice in and out of bed, on and off the toilet, into and out of a wheelchair, all to the stronger side, or walking practice inside the parallel bars, and stair practice with instructions to “lead up with the strong leg and down with the weak leg.” Often, devices such as hemi-walkers, quad- and single-point canes, grab bars by the bed and in the bathroom for transfers, and adapted tools for activities of daily living (ADLs), such as rocker knives, reachers, and other one-handed bathroom and kitchen devices, are prescribed for this individual to promote independence. (The advent of Velcro, as useful as it is in many realms of life, also contributes to this path to compensation.) However, in this effort to promote independence, PTs may be encouraging a bias of strengthening what is still working at the expense of what is not working or is working but with impairments on the more involved side, including the trunk. A similar list of concerns and the sequelae of secondary impairments as outlined in the example of the child who W-sits could be made for this individual. Over time, the overuse and dependence on the muscles, joints, and ligaments in the trunk and of the more involved arm and leg may lead to pain, fatigue, and skeletal deformities (Fig. 17.2). For example, chronic shoulder subluxation can lead to an overstretched capsule, overlengthened cervical and scapular muscles, impinged tendons and bursas at the shoulder, and pain. Chronic knee hyperextension can lead to overlengthened posterior knee capsular ligaments, joint surface deterioration, and shortening of the gastrocnemius–soleus muscle group. The effect of these alignments may guide the shoulder into further internal rotation and adduction leading to impingement syndromes, the hip into flexion and adduction and the ankle into plantar flexion and inversion causing further stress at these joints, and the trunk into thoracic flexion with lateral shortening. All of these changes lead to the individual’s center of mass (COM) being shifted over a smaller and less dynamic base of support (BOS). This posture may result in impaired balance and difficulty shifting weight over the BOS in postures such as sitting and standing and in movements such that the individual’s functions in activities such as walking in and outdoors, getting in and out of a car, swinging a golf club, and getting dressed for work all become compromised. Fig. 17.2 Carol, a woman poststroke whose case report appears in Unit V (A3) shows malalignment in standing that contributes to poor balance and ineffective movement through space. The client, the PT, and the involved family members must explore the possibilities for other movement solutions that still promote independence, in both the short and the long term, while also assisting CNS recovery from the stroke damage and the subsequent body system impairments the stroke caused. Clearly, for the individuals in the foregoing examples, the PT must focus on each ineffective or compensatory posture and movement the client makes or is likely to make. The PT may decide with the client and family to accept some compensations (fully or in part) and not accept others (within their control). Understanding past, present, and future postures and movements that each person with CP or poststroke uses or may use requires a deep working knowledge of effective, ineffective, and compensatory body system development and function, biomechanics, kinesiology, and the effects of posture and movement repetition on function. NDT-educated PTs view activity and participation as the desired outcomes for clients with stroke, traumatic brain injury (TBI), CP, and related neurodisabilities. This view shapes their entire practice, from initial information gathering and examination through intervention and home/school/work/leisure program suggestions. Because stroke, TBI, CP, and related neurodisabilities adversely affect the ability to produce all of the posture and movement requirements of function, repetitive, open-chained exercises using isolated muscle activity are usually insufficient in meeting activity and participation requirements. NDT-educated PTs focus instead on posture and movement requirements within specific functional tasks chosen by clients as outcomes. However, the principles of exercise learned in entry-level university education assist in intervention in the following ways: • The PT modifies the effects of gravity as appropriate, controls the effects of body and segmental position, provides support of the body segmentally and as a whole, and monitors demands on all body systems (i.e., neuromuscular, musculoskeletal, sensory, perceptual, cardiovascular, respiratory) while the client engages in participation, activity, and/or repetitions of functional postures and movements. • The PT progresses activity, building from simple postures and movements for the client to control and coordinate to postures and movements of greater complexity. • The PT includes practice and repetition, both for motor learning of participation and activity with the most effective postures and movements and for building endurance in body systems by increasing the level of challenge or interspersing rests as appropriate for each individual. • The PT monitors the client’s physiological responses to the physical work required. For example, a PT working with a 6-year-old child with CP (spastic diplegia) sets a session outcome for the child to step up a 3- to 5-inch-high curb or to step using forearm crutches. The PT knows that each time this particular child attempts a new skill requiring more complex strength and balance (and in this case, the fear of using crutches in a new way), his first choice of posture includes increasing upper thoracic flexion, increasing weight bearing through the crutches with his hands, increasing shoulder internal rotation, breath holding, and increasing LE stiffness with more hip adduction and internal rotation than he uses when he is confident in his performance. Strengthening and crutch use are skills PTs and PTAs learn in entry-level education, with faculty instruction and testing to ensure that the student monitors each skill for safety, correct procedure, and correct alignment. The activity outcome for this child requires much more than strengthening hip, knee, and ankle extensors concentrically to lift his body weight up the curb. The activity requires more than placing the crutches safely and properly. The PT and PTA following the PT’s plan of care add detailed declarative and procedural knowledge from the NDT Practice Model regarding the following: • Ensuring the client’s best body alignment in all body segments in the initial posture in front of the curb, with one foot placed up on the curb, and in the ending posture. • Ensuring the correct direction and amount of weight shifting needed to first unweight one LE, lift and place that LE on the curb step, shift weight onto that LE, and advance the trailing LE and crutches. • Coordinating the child’s posture and movement with respirations, and facilitating postures and movements that ensure effective respirations and continuous breathing throughout the activity of stepping up a curb. For this child, this coordination would include facilitating an upright trunk posture with active or active-assisted thoracic rotation and facilitating shoulder posture out of excessive internal rotation. • Including practice sessions that progressively increase difficulty of the task, taking into consideration all body systems (i.e., not simply stepping up a higher step, but setting up the environment to reduce fear, progressing from a large space to place crutches to a narrower space if needed, controlling the visual perceptual demands of the task, and altering verbal and physical cues as needed). • Ensuring practice of the more efficient postures and movements to complete the task while engaging this 6-year-old in activity commensurate with his age, cognitive, and attention needs. • Providing information to the child’s family for practice of the task that is safe and easy for the family to accomplish within their everyday routine and the child’s activities (asking them to provide verbal and physical cues within their roles as family members vs. “doing therapy”). One scenario could be that the PT sets up an environment where the child steps up a 2- to 3-inch-high step and then a 3- to 5-inch-high step with physical assistance as needed to shift weight correctly and safely. Then the PT provides physical assist as necessary to align the LEs in that child’s most efficient posture to use the extensors concentrically as he steps onto a platform with a large area. Simultaneously, the PT ensures a visually uncluttered environment and targets visual attention with a marker, such as colorful tape placed on top of the platform where his feet should step (Fig. 17.3). The PT creates a game based on knowledge that this child enjoys water play, handing him small plastic animals to place in his pockets, after which he ascends the step and places the animals in the “bathtub.” He descends the step to gather more animals. This game allows repetition of step/curb ascent and descent in a way that is engaging for the child. For a home practice activity, his mother is asked to place her hands on her son’s shoulders to provide contact guarding and guide the correct weight shift as he steps up with his crutches onto the threshold step between the garage and the kitchen each time the family comes home from a car trip.
17.1 Definition of Physical Therapy (Physiotherapy)
17.2 A Brief History of Physical Therapy and the Origins of Neuro-Developmental Treatment
17.3 Expertise and Contributions of Physical Therapists to NDT Practice
17.4 The Contributions of NDT to Physical Therapy
17.4.1 Problem-Solving of the Physical Therapist Using the NDT Practice Model: A Child with Cerebral Palsy
17.4.2 Problem-Solving of the Physical Therapist Using the NDT Practice Model: An Adult Poststroke

17.4.3 Exercise and Practice

Related posts:
 Neuroplasticity and Recovery
Neuro-Developmental Treatment Practice and the ICF Model
Report A6 Achieving Functional Outcomes with Neuro-Developmental Treatment for Chronic Stroke
Report A5 Examination, Evaluation, and Intervention with an Individual Poststroke with Cognitive Impairments
Report A4 Addressing the Primary and Secondary Impairments of a 20-Year-Old Man with Traumatic Brain Injury
Neuro-Developmental Treatment Intervention—A Session View
Neuroplasticity and Recovery
Neuro-Developmental Treatment Practice and the ICF Model
Report A6 Achieving Functional Outcomes with Neuro-Developmental Treatment for Chronic Stroke
Report A5 Examination, Evaluation, and Intervention with an Individual Poststroke with Cognitive Impairments
Report A4 Addressing the Primary and Secondary Impairments of a 20-Year-Old Man with Traumatic Brain Injury
Neuro-Developmental Treatment Intervention—A Session View
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


