Chapter 11 Therapeutic Epidural Injections
Interlaminar and Transforaminal





 Transforaminal epidural techniques place the medication in the anterior epidural space nearer the putative site of pathology.
Transforaminal epidural techniques place the medication in the anterior epidural space nearer the putative site of pathology.


 Patient response should be based on outcome of each injection, and proscriptive use of specific numbers of injections (e.g., three epidurals) is not evidence based.
Patient response should be based on outcome of each injection, and proscriptive use of specific numbers of injections (e.g., three epidurals) is not evidence based.
Introduction
The use of therapeutic epidural injections for the treatment of sciatica with back and leg pain dates back approximately 80 years. Initially, therapeutic epidurals were predominately transsacral (caudal) injections of local anesthetics such as procaine.1 After the introduction of corticosteroids into clinical practice,2 researchers in Europe were the first to inject corticosteroids into the epidural space.3,4 The techniques of administration have gradually been modified, with early use of higher volume caudal epidural injections eventually being largely replaced, first by level-specific interlaminar epidural injections and second by transforaminal epidurals performed with fluoroscopic guidance. Despite the increasing sophistication and advances in the techniques of steroid injection, a number of authors still question the role of these injections for the therapy of sciatica. In particular, two physician specialties (neurology and occupational medicine) have published guidelines or reviews suggesting that these injections are performed too often with uncertain results.5,6 Other authors are beginning to examine the role of alternate compounds such as etanercept for the treatment of sciatica based on the underlying pathophysiology.7 Finally, a recent head-to-head trial of several conservative treatments (including injections in some) compared with surgical therapies was performed demonstrating the superiority of surgery, at least in the first year.8 This trial augmented the previous large-scale trials comparing surgical with nonsurgical therapies.9,10 This chapter discusses the current role of therapeutic epidural injections.
Basic Science
Radiculopathy is most commonly associated with intervertebral disc herniation and likely includes two distinct pathways: mechanical compression and cytokine-mediated radiculitis.11 Mechanical impingement may induce poor tissue oxygen delivery to the spinal (radicular) nerve, resulting in an inadequate nutritional supply and decreasing the vascular perfusion to critical levels. Interestingly, however, mechanical compression alone may not result in pain.12,13 Radiculopathy describes neurological conduction loss (sensory or motor) occurring secondary to mechanical impingement or compression (e.g., disc protrusion, herniation, or extrusion) pressing on the spinal nerve in the foramina. Other common causes of radiculopathy include spondylosis, vertebral subluxation, and ligamentum flavum hypertrophy or thickening.14 Abnormal nerve conduction may manifest as sensory loss, depressed spinal reflexes, or motor deficits. Radicular pain may occur concomitantly with radiculopathy or separately. The pain is thought to be an inflammatory phenomenon induced by neurochemical products such as cytokines. Cytokines are produced by spinal glia. They include tumor necrosis factor-α (TNF-α) and several interleukins. Herniated nucleus pulposus may induce the release of such inflammatory mediators, leading to a chemical radiculitis. Olmarker et al15 found that the application of a homogenate of disc material onto porcine cauda equina induced functional and morphologic changes in those nerves. Then Igarashi and colleagues16 reported that in a rat model, TNF-α applied to the dorsal root ganglia produced functional and morphological changes that were identical to that seen with nucleus pulposus material. Burke et al17 found increased levels of the inflammatory cytokines interleukin-6 (IL-6) and IL-8 in disc material taken from patients with known disc disease. Finally, further study produced compelling evidence that TNF-α inhibitors could reduce the histological and functional changes caused by nucleus pulposus material. These studies cemented the concept that TNF-α and other cytokines were causative agents in the development of radiculitis and further suggested an entirely new pharmacological treatment strategy for patients with sciatica.18
Discogenic pain is another pathological condition for which epidural therapies are occasionally tried. Discogenic pain is unlike radicular pain in that the patient will predominately complain of low back pain without significant leg involvement that is exacerbated by the sitting position, spinal flexion, heavy lifting, or other stresses. The intervertebral disc is a very poorly vascularized structure that receives nutrients primarily by diffusion. Intervertebral disc innervation is complex, arising primarily from nerve ingrowth through the vertebral endplate into the outer third of the disc annulus. Nerve fiber types in the annulus fibrosis are peptidergic, using neurotransmitter substances such as calcitonin gene-related peptide. Nerve fibers are small and follow new blood vessels.19
Indications and Contraindications
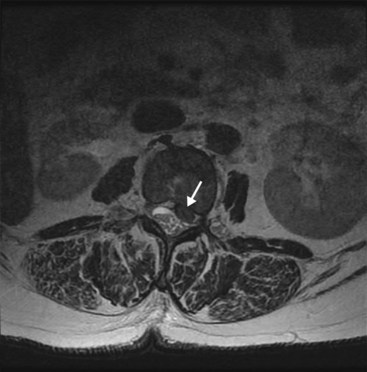
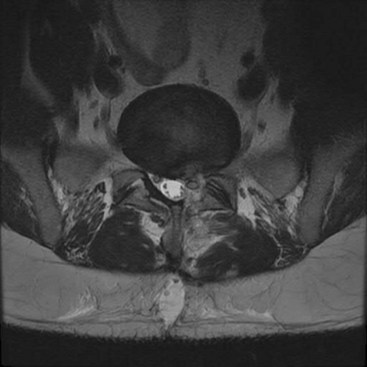
Therapeutic epidurals are generally used in three major instances: (1) for the symptomatic treatment of radicular pain secondary to an intervertebral disc herniation, protrusion, or extrusion causing a combination of back and leg pain in a characteristic dermatomal pattern (Fig. 11-1); (2) spinal stenosis presenting with symptoms of neurogenic claudication, radicular pain, or mixed pain (Fig. 11-2); and (3) postoperative back and leg pain caused by recurrent disc material, granulation tissue or scarring, or other causes (Fig. 11-3). In some cases, therapeutic epidural injections may also be performed in cases of discogenic pain or for tumor-related nerve pain when a radicular syndrome is manifested by the tumor growth into the foramen or around the exiting spinal nerve (Fig. 11-1). How these therapeutic procedures are applied is also somewhat variable depending on regional variations in the use of initial conservative therapies, the specialty of origin of the managing clinician, and the availability of clinicians capable to do therapeutic epidurals. However, population-based examinations of therapeutic epidural injections have not demonstrated any long-term advantage to their use in terms of reduced surgical volumes or enhanced functionality.20

Spinal stenosis is most commonly acquired but can be congenital. Large studies are lacking for results of therapeutic epidural injections. The natural history of spinal stenosis is reassuring, however. Johnsson and colleagues21 demonstrated that older patients with spinal stenosis commonly presented with low back pain (100%), claudication (75%), radicular pain (12.5%), and mixed symptoms (12.5%). Interestingly, the patients with spinal stenosis did not appear to worsen significantly over a 4-year period, with equal numbers showing improvement as progression.
Patients with worse clinical and functional symptoms most often had surgical laminectomy without fusion. At 8 to 10 years, the patients treated with either surgical or nonsurgical approaches had similar rates of satisfaction with current state, back pain incidence, and symptom improvement. Patients with initial surgical treatment had better leg pain and functional status. Overall, the results suggested that patients may be optimally managed in a shared decision model.22
Imaging
Numerous studies have demonstrated that a high percentage of patients who are clinically asymptomatic will have significant findings on magnetic resonance imaging (MRI).23 In most cases, the MRI should be read before proceeding with the injection and is mandatory before cervical epidurals. The size of the spinal canal, presence of intervertebral disc protrusion or extrusion, any neural impingement, presence of degenerative changes, or any possible abnormality in the path of the proposed needle placement will need to be accounted for.
The high rate of false-positive scans mandates an approach to patient evaluation that requires a large degree of concordance among the imaging, electrodiagnostic testing, the history, and the physical examination. In some cases, a diagnostic spinal nerve injection to independently verify which root is involved in pain generation is requested before surgical intervention. Studies performed more than 2 decades ago were the first to suggest that image guidance could significantly improve the accuracy of epidural administration of medication.24 Johnson et al25 later published 5489 consecutive injections performed with fluoroscopic guidance with contrast injection. Their results suggested an extremely safe conduct of these outpatient injections could be accomplished with a high degree of accuracy and precision.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


