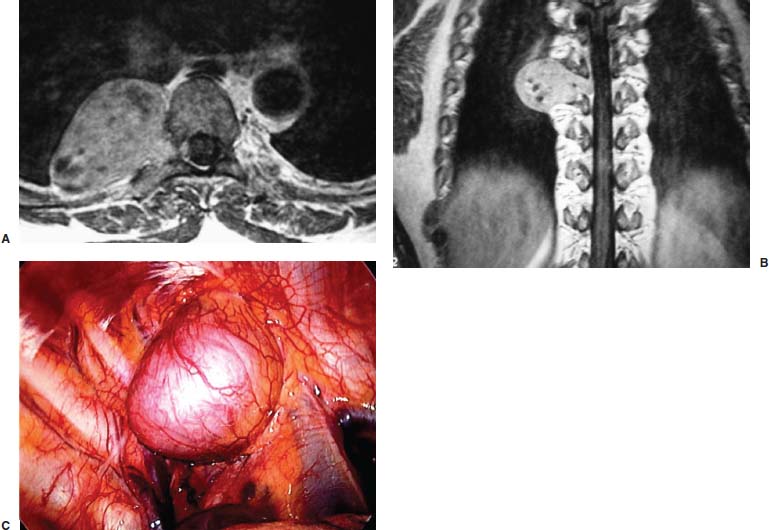
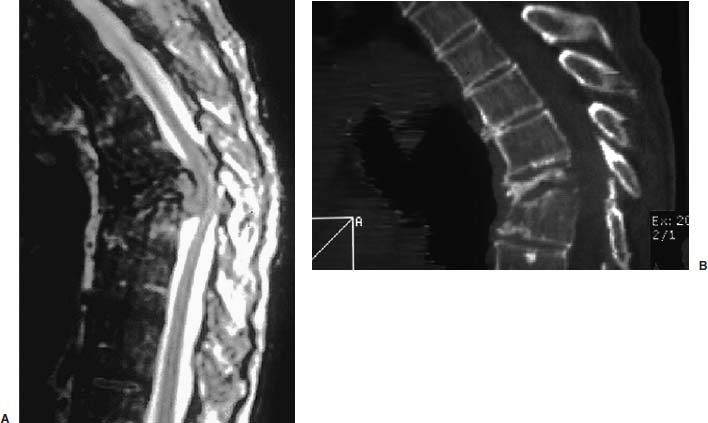
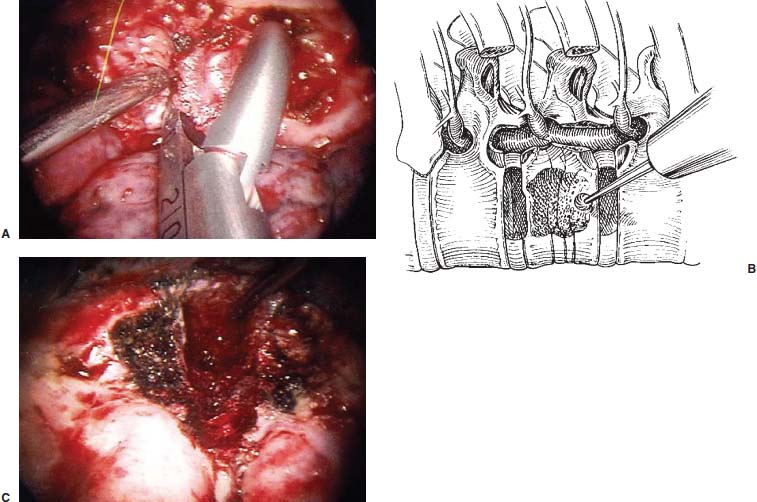
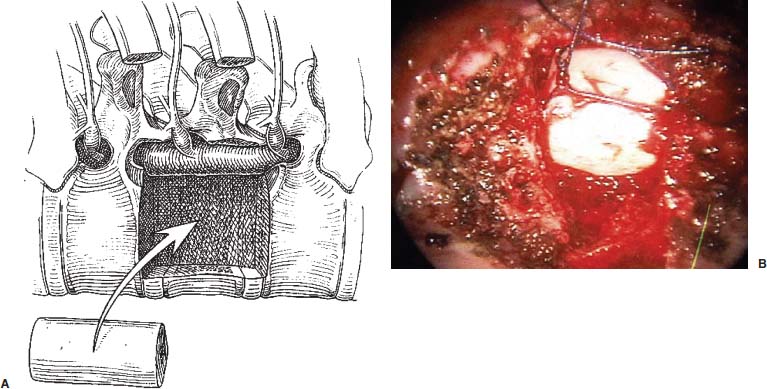
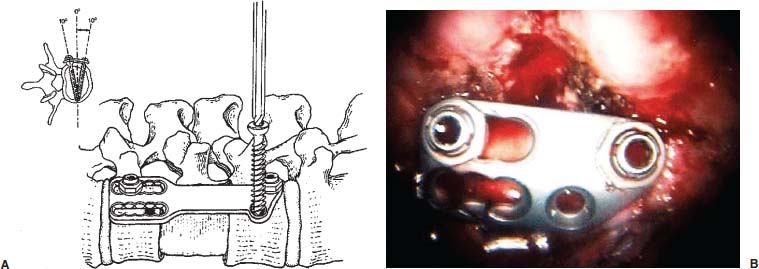
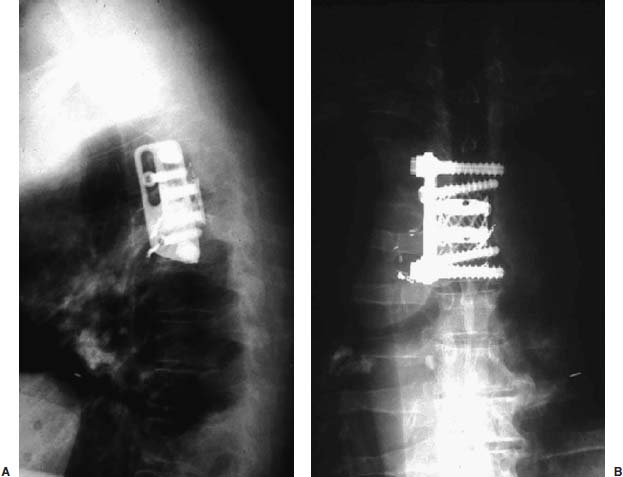
Thoracoscopic spinal surgeries for neurogenic and vertebral tumors are advanced procedures that are beyond the basic procedures of sympathectomy and the more complex procedures of diskectomy for spinal cord and spinal nerve decompression. The advances in endoscopic thoracic spinal procedures described in the previous chapter allow these techniques to be used for significantly more complex spinal disorders, including resection of neurogenic tumors and reconstruction of vertebral tumors. The advantages of thoracoscopy over thoracotomy that have been described for the treatment of both spinal and nonspinal disorders are well known. Although thoracoscopic procedures have altered the treatment paradigm for many of these lesions, significant limitations to these procedures remain, particularly for the inexperienced endoscopic spinal surgeon. The procedures described here require the surgeon to have a working familiarity with more fundamental thoracoscopic procedures as a prerequisite to perform these more complex procedures with appropriate safety and efficacy. In this chapter, we will describe the indications and techniques for thoracoscopic resection of neurogenic tumors and vertebral tumors. Indications Neurogenic Tumors The most common neurogenic tumors in the thoracic spine are schwannomas and neurofibromas; less frequently, there are other tumors of nerve origin arising from segmental intercostal nerves. They are typically benign tumors and are rarely malignant, presenting as the classic “dumbell” tumor, with a smaller component in the spinal canal causing spinal cord compression with a larger intrathoracic component (Fig. 13–1A,B). These tumors can also present with chest wall pain due to spinal nerve compression or may be discovered incidentally with a routine chest radiograph. Strategies for surgical resection of these tumors depend entirely on their anatomic location. Tumors that are found exclusively within the chest cavity arising from an intercostal nerve can be removed with thoracic endoscopic techniques (Fig. 13–1C). Tumors that extend into the neural foramen without an intraspinal component can still be removed with a thoracoscopic procedure; however, that portion of the tumor that extends into the spinal canal must be removed with a posterior laminectomy exposure and excision. The intraspinal tumor must also be evaluated as to whether the lesion is intradural or extradural. This can be determined with a postmyelography CT scan that will assist in defining the location in relation to the thecal sac. Tumors that do not extend into the spinal canal can be treated solely with an endoscopic procedure. If the tumor extends into the spinal canal, then a combined transthoracic and posterior tumor excision can be performed. We have performed these procedures simultaneously in a lateral position, which can expedite the procedure. Vertebral Tumors Vertebral tumors are primary or secondary neoplasms that affect the vertebral body and may result in either vertebral collapse or tumor mass that compresses the spinal cord. The most common vertebral tumors are metastatic, and primary vertebral tumors are relatively rare (Fig. 13–2). These tumors, which previously required a thoracotomy, are potential candidates for thoracoscopic resection and reconstruction. They typically have a slowly progressive presentation pattern with onset of continuous unremitting pain. Neurologic deficits usually occur later in the clinical course and only rarely require urgent surgical intervention. These lesions have often been irradiated and have a wide range of variability in radiation responsiveness that generally depends on the tissue type and biologic behavior. FIGURE 13–1 (A,B) Axial T2 MRI showing nerve sheath tumor with intrathoracic extension. (C) Thoracoscopic view of nerve sheath tumor. Imaging for Thoracic Spinal Tumors Imaging for thoracic spinal neoplasms is essential for determining whether a lesion can be treated successfully with a thoracoscopic procedure. Magnetic resonance imaging (MRI) is the ideal method for surveying the thoracic spine due to superior soft tissue definition with orthogonal views to visualize the spinal cord, vertebral lesions, and adjacent anatomy that may include extension of the neoplasm that affects surgical decision making. Because bony anatomy is not as well defined with MRI techniques, CT (Fig. 13–2B) is useful to demonstrate the bony architecture of the vertebral column. Neurogenic tumors typically do not invade the vertebral column, but they can erode and enlarge the neural foramen where it exits the nerve in a classic dumbbell shape. Vertebral tumors from metastases or primary bony tumors cause destruction of the bony architecture that requires definition with CT imaging to determine the extent of tumor involvement and what tumor resection and reconstruction will be required. Most cases of thoracic spinal tumors require both MRI and CT scans to define the anatomic details fully for either an open or a thoracosopic procedure. Plain radiographs of the thoracic and lumbar spine are always obtained preoperatively to determine deformity and for verification and comparison of intraoperative radiographs to confirm the level(s) operated. FIGURE 13–2 MRI (A) and CT (B) showing metastatic vertebral tumor causing compression fracture with kyphotic deformity. Surgical Procedure Description of Procedure Thoracoscopic spinal procedures for diskectomy and sympathectomy have been well described previously and provide the basic thoracoscopic spinal surgical skills necessary to perform these more complicated procedures. The procedure begins with induction of general anesthesia and placement of a double lumen endotracheal tube for ventilation of the opposite lung during the operation. The patient is placed in a lateral position, with the operated side of the spinal column facing upward. The arm is held in an “airplane” holder to expose the chest wall. A preliminary anteroposterior chest radiograph is then obtained for localization of the spinal level and the portal sites. This assists in precise placement of the portal sites prior to prepping and draping, with the thoracoscope portal placed in the chest cavity perpendicular to the level of the pathology in the posterior midaxillary line. Two additional working ports are established in the anterior/midaxillary line rostral and caudal to the operated level. Soft portals are used to help reduce the incidence of intercostal nerve injury. Initial thoracoscopy includes retraction of the lung anteriorly that is facilitated by rotation of the operating table. The exact spinal level is then identified by placing a localizing needle into the disk spaces adjacent to the level of interest and obtaining another radiograph. This may be obviated in large neurogenic tumors that are clearly visible within the chest cavity. Vertebral Tumor Removal and Reconstruction A vertebral tumor resection usually requires a vertebrectomy procedure and exposure by reflecting the parietal pleura widely over the site of the pathology to expose the vertebra, rib heads, and disk spaces. The segmental vessels crossing in the midportion of the vertebral body can be coagulated and divided with clips and/or cautery. The rib head at the resection level is subsequently removed with the pneumatic drill to expose the pedicle, which is removed to expose the spinal canal Fig. 13–3). A vertebrectomy to remove the tumor is then completed with curettage or a pneumatic drill (Fig. 13–4). The adjacent level disks can be removed with standard dissection techniques. The decompression is continued until the ventral aspect of the spinal cord is visualized. The anterior longitudinal ligament can be removed with a blunt tip probe and divided with Kerrison rongeurs to expose the dura. Bone bleeding is controlled with bone wax, and epidural hemostasis is achieved with Gelfoam and/or bipolar cautery. Reconstruction of a vertebrectomy defect can be accomplished with either a bone graft or a titanium mesh cage, depending on the pathology (Fig. 13–5). We typically use a cage for metastatic tumors and either an autograft or an allograft for infectious cases that will progress to fusion. The vertebral implant is inserted into the chest through a slightly enlarged portal site. Instrumentation with a lateral plate or screw-rod construct can be used to secure the graft in place (Fig. 13–6). Additional portals may be required to place instrumentation with screw trajectories across the vertebral bodies and assemble a plate or screw-rod construct. FIGURE 13–3 (A,B) Exposure and removal of the rib head for exposing the pedicle. FIGURE 13–4 (A–C) Intraoperative photos and artist’s depiction demonstrating a vertebrectomy. FIGURE 13–5 (A,B) Reconstruction with bone graft. A spinal tumor resection of a neurofibroma usually does not require significant bone removal that involves vertebrectomy because these tumors are usually distinctly separate from the bony structure of the vertebra. The vertebra and rib may be eroded with an enlarged foramen that is seen in the classic dumbbell-shaped tumor. These tumors require exposure by opening the pleura widely to expose the full extent of the lesion. Small tumors can be removed en bloc, but larger tumors are removed by internal debulking with pituitary rongeurs, followed by dissection and mobilization of the capsule with surgical techniques similar to open procedures. Hemostasis in the tumor resection cavity can be achieved with bipolar cautery. FIGURE 13–6 (A,B) Addition of lateral plate fixation. A number 20 French chest tube is inserted and externalized through one of the portals. The portals are removed, and the incisions are closed in layers. Sterile dressings are subsequently applied. The chest tube is placed to suction in the operating room and to water seal in the recovery room; it is usually removed within 24 to 48 hours. Thoracoscopy was initially introduced as a diagnostic tool for evaluation of pleural disease but has expanded greatly over the years now to include treatment of thoracic disk herniations, sympathectomies, vertebral biopsies, spinal deformities correction, and, lastly, corpectomies associated with trauma or tumor followed by reconstruction and stabilization. Over the past 2 decades, several clinical studies have found significant advantages of thoracoscopy over thoracotomy in terms of reduced postoperative pain, reduced intensive care unit and hospital stays, shortened recovery time, faster return to activity, and lower complication rates. Overall, the advantages of the thoracoscopic approach are numerous; however, when applied to cases of thoracoscopic tumor resection, reconstruction, and stabilization, a surgeon must have the added working familiarity with more fundamental thoracoscopic procedures as a prerequisite to perform these more complex cases. FIGURE 13–7 (A,B) Postoperative radiographs after thoracoscopic tumor vertebrectomy, cage reconstruction, and fixation.
13

Thoracoscopic Management of Spinal Tumors


< div class='tao-gold-member'>
Related posts:
 Endoscopic-Assisted Transoral Odontoidectomy
Endoscopic-Assisted Transoral Odontoidectomy
 Image-Guided Endoscopic and Minimally Invasive Spine Surgery
Image-Guided Endoscopic and Minimally Invasive Spine Surgery
 Combined Prone Position Thoracoscopic Anterior Release and Posterior Instrumentation for Deformity Surgery
Combined Prone Position Thoracoscopic Anterior Release and Posterior Instrumentation for Deformity Surgery
 Anterior Endoscopic Cervical Microdiskectomy
Anterior Endoscopic Cervical Microdiskectomy
 Nucleoplasty
Nucleoplasty
 Minimally Invasive Instrumentation, Correction, and Fusion of Primary Thoracic and Thoracolumbar Scoliosis
Minimally Invasive Instrumentation, Correction, and Fusion of Primary Thoracic and Thoracolumbar Scoliosis



