Traumatic Lesions of the Brain
Juan C. Troncoso
Olga Pletnikova
SUBARACHNOID HEMORRHAGE
Subarachnoid hemorrhage is the most common pathologic consequence of head trauma. This hemorrhage is frequently multifocal, and its distribution is variable. Generally, it is more prominent over the convexity of the hemispheres (Fig. 7.1), in contrast to the hemorrhage from a berry aneurysm, which is more abundant at the base of the brain. Initially, subarachnoid hemorrhages have the dark-red color of fresh blood (e-Fig. 7.1), but subsequently, as hemoglobin is broken down to hemosiderin, the color turns to a golden brown (Fig. 7.2). A potential long-termcomplication of subarachnoid hemorrhage is blockade of normal cerebrospinal fluid circulation and the eventual development of communicating hydrocephalus.
Subarachnoid hemorrhage is a common neuroimaging finding in cases of traumatic brain injury (TBI) admitted to the hospital. The neuropathologist should be aware that at times, however, in cases of acute hypoxic-ischemic encephalopathy, computed tomography images lead to a false-positive diagnosis of subarachnoid hemorrhage.1
CORTICAL CONTUSIONS
These lesions represent bruising of the brain, most frequently of the cerebral cortex, because of impact against the skull (Figs. 7.3, 7.4 and 7.5, e-Fig. 7.2). Most contusions, but not all, are hemorrhagic (Fig. 7.6). Cortical contusions may give rise to focal neurologic manifestations and/or seizures.
LACERATIONS OF THE BRAIN
Wounds or tears in the parenchyma of the brain result from high mechanical stress and frequently are the result of skull fracture (Figs. 7.7 and 7.8). Lacerations may also result from the shearing forces secondary to acceleration/deceleration, such as those involving the corpus callosum (Figs. 7.6 and 7.7A). In instances of traumatic hyperextension of the head and neck, lacerations of the brainstem, either at the pontomesencephalic (Fig. 7.9) or pontomedullary junctions, are not uncommon.
AXONAL SHEARING
Invisible to the naked eye, axonal shearing is a common lesion of cerebral white matter that occurs, in particular, in acceleration/deceleration injuries (e.g., automobile accidents). Axonal injury is a major culprit for the cognitive and motor deficits that characterize the aftermath of trauma. The microscopic hallmark of axonal shearing is the presence of axonal balloons, which are the proximal stumps of severed nerve fibers. These axonal balloons are not present immediately after the injury, but can be detected in approximately 24 hours on hematoxylin and eosin stains (Fig. 7.7B). Immunostains with antibodies against neurofilaments (Figs. 7.7C and D) or beta amyloid precursor protein (APP) (Fig. 7.7E) are the best method to demonstrate axonal balloons. An important caveat, however, is that axonal balloons are not specific for trauma, because they are present in axonal injuries of other causes (e.g., infarcts).
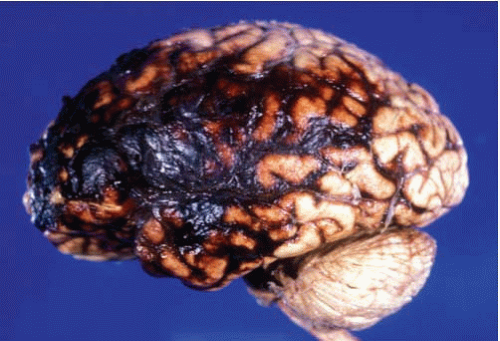 FIG. 7.1. Fresh traumatic subarachnoid hemorrhage over the left frontal, temporal, and parietal lobes. |
TRAUMATIC HEMORRHAGES OF THE BRAIN
Traumatic hemorrhages of the brain (Figs. 7.8 and 7.10) can be single or multiple, and their distribution is different from the hemorrhages associated with high blood pressure. Amyloid deposition in the cerebral blood vessels of older individuals makes them more prone to traumatic hemorrhages. A site of predilection for traumatic hemorrhages is the cerebral white matter. The ventricular system is also frequently the site of traumatic hemorrhages, most
of the time associated with other traumatic brain lesions, although occasionally hemorrhage may be the only sign of injury.
of the time associated with other traumatic brain lesions, although occasionally hemorrhage may be the only sign of injury.
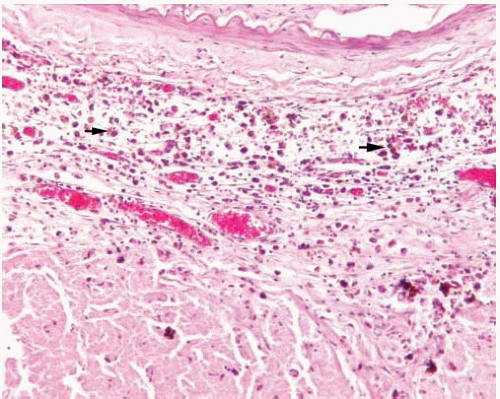 FIG. 7.2. Photomicrograph of an old subarachnoid hemorrhage. the subarachnoid space contains hemosiderin-laden macrophages (black arrows). |
MECHANISMS OF HEAD INJURY AND PATTERNS OF BRAIN LESIONS
Specific patterns of TBI have been recognized by neuropathologists for many years; however, the mechanisms and the physics underlying these various patterns remain unclear. The paradoxical nature of contrecoup contusions has intrigued and fascinated physicians and scientists for centuries, as revealed by the offer of a prize by the Academie Royale de Chirurgie in Paris in 1766 for “établir la théorie des contrecoups dans les lésions de la tête et les conséquences qu’on peut en tirer” (to establish the theory of contrecoups in lesions of the head and its implications).2 In this chapter, we will follow a descriptive approach, discussing in detail those patterns of contusions that are most common in forensic neuropathology, including those present in blunt trauma, falls, and vehicular accidents. Although traumatic brain lesions are usually the consequence of a combination of mechanisms, the three most common mechanisms of TBI are discussed separately for didactic purposes.
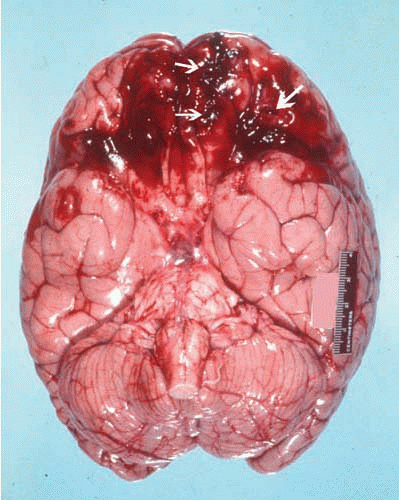 FIG. 7.3. This fresh brain shows traumatic subarachnoid hemorrhage and contusions (white arrows) of the orbitofrontal regions in a subject who died of a fall with impact on the back of the head. Note the lack of hemorrhage in the basal cisterns and around the circle of Willis, findings usually seen in ruptured aneurysms. |
Lesions Caused by Blunt Trauma to the Head
Blunt trauma to the head is characterized by scalp contusion or laceration, skull fracture, and underlying contusion or laceration of the brain parenchyma, all at the point of the impact or coup lesions (Fig. 7.8). Epidural and subdural hemorrhages on the same side of the blow also occur frequently. Figure 7.11 illustrates the scalp/skull lesion in a case of blunt trauma to the head with a baseball bat. The skull in this case showed a fracture under the scalp contusion. The brain parenchyma under the point of impact showed a large laceration, and subtle petechial hemorrhages highlight contusions on the site opposite to the impact. Therefore, this constitutes a contrecoup contusion. In contrast to the contrecoup lesions seen in falls (see below), in blunt trauma, the contrecoup lesion is minuscule compared with the lesions at the site of impact (coup) (Fig. 7.8).
When the blunt trauma to the head is caused by a massive object, such as a falling tree, the lesions described above are accompanied and overshadowed by multifocal petechial hemorrhages of the parasagittal cerebral white matter, corpus callosum, and rostral brainstem, akin to those seen in victims of traffic accidents and in which the effect of acceleration/deceleration predominates (see below)3 (Fig. 7.12).
Case 7.1
A 52-year-old man was part of a crew attempting to clear a tree that extended over a road. He was cutting a tree with a power saw when the tree split and fell, striking his unprotected head and pinning him to the ground. He had no signs of life at the scene, cardiopulmonary resuscitation was initiated, and he was pronounced dead on arrival at the hospital.
Gross examination of the body at autopsy revealed an avulsed left ear, a large transverse laceration of the left temporal parietal scalp extending to the calvaria, bleeding from the right ear, and a basal skull fracture involving the left temporal bone. External examination of the brain revealed subarachnoid hemorrhage over the frontal parietal convexities bilaterally, a minimal and superficial left temporal parietal hemorrhagic contusion, and hemorrhagic contusions over the left base and orbital frontal region bilaterally. No herniation had occurred. On coronal sectioning, prominent midline white matter hemorrhagic lesions were noted. These lesions included clusters of petechial hemorrhages in the parasagittal white matter, in the anterior frontal white matter extending through the centrum semiovale to the gyri recti and temporal lobe isthmi, and in the caudate, putamen, corpus callosum, and amygdala (Fig. 7.12). Microscopic examination revealed perivascular hemorrhages of the white and gray matter. Immunohistochemistry for phosphorylated neurofilament protein did not reveal axonal changes.
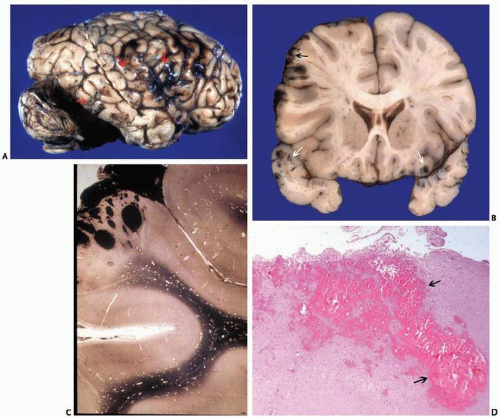 FIG. 7.4. Fresh hemorrhagic contusions. A. Fixed brain showing hemorrhagic contusions of the right frontal, parietal, and temporal lobes (arrows). B. Coronal section of a fixed brain showing fresh hemorrhagic cortical contusions (arrows) of the left frontal lobe, orbitofrontal regions, and both temporal poles. C. Low-magnification photomicrograph demonstrating fresh cortical contusion and subarachnoid hemorrhage. D. Photomicrograph of a fresh cortical hemorrhagic contusion (arrows). Note the edema of the neuropil surrounding the hemorrhage. |
Lesions Caused by Falls (Coup-Contrecoup)
One of the most consistent observations in forensic neuropathology is that individuals who fall and hit the back of the head suffer extensive contusions of the poles and inferior surfaces of frontal and temporal lobes, and lesser or no lesions of the brain at the site of impact. These lesions opposite to the site of impact are known as contrecoup (Figs. 7.13 and 7.14). At times, a cerebellar or occipital contusion marks the site of impact; this is the coup injury (Fig. 7.14). These injuries may or may not occur, but when they do, they are invariably smaller than the contrecoup injuries. This characteristic “coup-contrecoup” pattern of brain lesions in falls was recognized as early as in the Renaissance by French pathologists and has been corroborated by many subsequent studies and publications.2, 4, 5, 6, 7 Figures 7.14, 7.15 and 7.16 illustrate this type of injury. The typical history is that of a subject who falls from the standing position and suffers a single impact, usually on the back of the head. The point of impact ismarked by injury of the scalp, ranging from a subtle bruise to a laceration. Even if no external scalp lesion is found, a subgaleal hemorrhage may be present. Old orbitofrontal and temporal contrecoup injuries, such as those in Figures 7.15 and 7.16, are common findings in forensic autopsies. This indicates that many of the individuals who suffer this type of injury survive for many years, although many may suffer from seizures. Because the contrecoup injuries frequently involve the prefrontal cortex, a region critical for executive functions, many of these individuals may also have neurobehavioral deficits.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


