Fig. 14.1
Midline sagittal T2-weighted MRI images from 8-month-old (top) and 8-year-old (bottom) Cavalier King Charles spaniels with Chiari-like malformation and syringomyelia. The 8-year-old dog is asymptomatic and syringomyelia was identified as part of a programme of screening breeding stock. The 8-month-old dog has a more obvious cerebellar vermis herniation (arrow) and a holocord syrinx (asterisk). This dog had clinical signs of neuropathic pain including phantom scratching of the shoulder region
14.2 Pathophysiology
Chiari-like malformation is characterised by disparity in volume between the caudal cranial fossa and its contents, so that the cerebellum and brainstem are herniated into or through the foramen magnum. Brachycephalicism and miniaturisation are risk factors for Chiari-like malformation (Schmidt et al. 2011). The condition is most commonly reported in toy breed dogs , in particular Cavalier King Charles spaniels, King Charles spaniels, Griffon Bruxellois , Affenpinschers, Yorkshire terriers, Maltese, Chihuahuas, Pomeranians and Papillons. Partly because of its popularity as a pet, the Cavalier King Charles spaniel is overrepresented (Fig. 14.2). Chiari-like malformation may also be seen in cats and is again more common in brachycephalic varieties such as the Persian.

Fig. 14.2
Left: Cavalier King Charles Spaniel. Right: Griffin Bruxellois (Picture courtesy of Henny van de Berg)
Brachycephaly in dogs and cats is a consequence of selecting for juvenile characteristics of flattened face and a ‘domed’ or ‘apple’ head (Stockyard 1941). This rounding of the top of the skull is actually bony compensation for basicranial shortening and in reality breeders are actually selecting for craniosynostosis (Table 14.1). Brachiocephalic breeds have early closure of the spheno-occipital synchondrosis, and in Cavalier King Charles spaniels, this closure occurs even earlier (Schmidt et al. 2013). Dog breeders generally strive to produce dogs which adhere strictly to a breed standard.1 Many breed standards were formulated in the nineteenth or early twentieth century, and registered pedigree dogs can be traced back to foundation stock from this time. Closed stud books ensure that no new genetic material is introduced. Only a small subset of each generation of dogs is used for breeding, and certain males produce a disproportionate number of offspring. This means that many breeds have very small effective population sizes and little genetic diversity. Although this has the advantage of ensuring the desirable appearance, it also means that spontaneous deleterious mutations can become widespread in a population. In addition, to improve success in the show ring, breeders may select for more extreme variations of the breed standard, which may be predisposed to disease and or discomfort (Fig. 14.3).
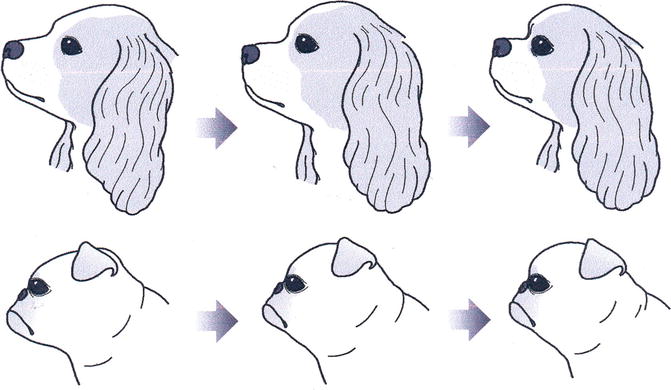
Table 14.1
Comparison between features of Crouzon syndrome and the breed standard for the Griffon Bruxellois
Features | Crouzon syndrome (branchial arch syndrome) | Breed standard |
|---|---|---|
Griffon Bruxellois | ||
Skull | Brachycephaly (short and broad head) | Broad head, with rounded and often domed skull |
Head large in comparison to body | ||
Ears | Low-set ears and high prevalence of ear canal malformations | Semi-erect, high set, the smaller the better |
Eyes | Exophthalmos (bulging eyes due to shallow eye sockets after early fusion of surrounding bones) | Largea and wide spaced eyes |
Hypertelorism (greater than normal distance between the eyes) | Showing white in the corner of eyes (lateral strabismus) considered desirable by some | |
Lateral strabismus | ||
Nose | Psittichorhina (beak-like nose) | Nose placed between the eyes and as short as possible |
Chin | Concave face and protruding chin because of insufficient growth of the upper jaw (hypoplastic maxilla) | Lower jaw curves upwards and should protrude beyond the upper jaw |
Fig. 14.3
How the Cavalier King Charles spaniel (top) and Griffon Bruxellois (bottom) head shapes have altered since the 1980s (left). A tendency to breed with dogs that are at the extremes of breed standards, or that display characteristics that are slightly bigger, better or more ostentatious than the dogs currently enjoying success in the show ring, will gradually produce dogs that are increasingly extreme. The modern Cavalier King Charles spaniel (upper right) typically has a shorter nose, a more pronounced ‘stop’ (i.e. a more acute angle between the skull and the nasal bone near the eyes), wider spacing between the eyes with the top of the head being broader and more domed. The modern Griffon Bruxellois (lower right) often has a shorter muzzle with a more domed skull with a more an ‘open face’, i.e. eyes that are larger and wider apart giving the dog a more appealing expression (Picture concept and expert opinion from Mrs Lee Pieterse ‘Statuesque’ Kennel, Sydney Australia, ANKC judge for all Toys and Terriers)
Brain size is not necessary correlated with body weight in domestic dogs; the ratio of brain size to body weight is larger in miniature compared to large breeds (Roberts et al. 2010). Brachycephalic dogs have considerable brain reorganisation, with the longitudinal axis of the brain adopting a more ventral orientation and the olfactory lobe shifting to a more ventral position (Roberts et al. 2010). Chiari-like malformation in the dog is characterised by extreme brachycephalism (Schmidt et al. 2011) combined with a disproportionately large brain (Cross et al. 2009).
The characteristics of Chiari-like malformation have been most studied in the Cavalier King Charles spaniel where the condition is almost ubiquitous within the breed (Knowler et al. 2011). Compared to some brachycephalic dog breeds, the Cavalier King Charles spaniel has a shorter braincase in relation to width (Schmidt et al. 2011), and compared to Cavalier King Charles spaniels without syringomyelia, syringomyelia-affected Cavalier King Charles spaniels have a shallower and smaller volume caudal cranial fossa (Carrera et al. 2009; Driver et al. 2010a). In the Griffon Bruxellois, Chiari-like malformation is characterised by shortening of the basicranium and supraoccipital bone, with a compensatory lengthening of the cranial vault, especially the parietal bone (Fig. 14.4) (Rusbridge et al. 2009). It has been suggested that, as the skull base is shortened, the developing forebrain is accommodated by lengthening of the other skull bones; however, insufficiency of the caudal cranial fossa bones (basioccipital and supraoccipital) means there is inadequate space for the hindbrain.
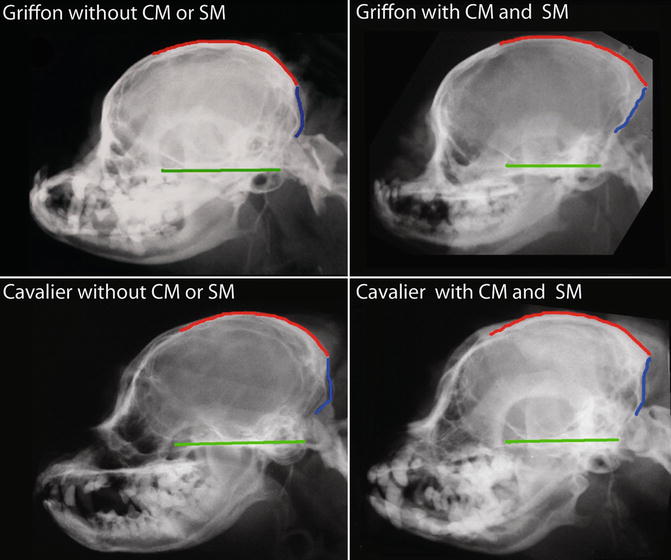
Fig. 14.4
Skull comparisons between Cavalier King Charles spaniels and Griffon Bruxellois with and without Chiari-like malformation or syringomyelia. Red approximates outline of parietal and inter parietal bone. Blue approximates outline of supraoccipital bone. Green approximates the basicranium. Note that with Chiari-like malformation (CM) and syringomyelia (SM), the basicranium shortens. In addition the supraoccipital bone is shorter and straighter, and there is an apparent compensatory lengthening of the parietal bone
The relative size of the brain is also important. The absolute and relative volume of the cavalier King Charles spaniel skull is similar to other brachycephalic toy dog breeds, but cavalier King Charles spaniels have a greater ditto volume of parenchyma within the caudal cranial fossa. Their brain parenchymal volume is approximately equal to that of the Labrador Retriever, a mesaticephalic breed which is two to three times the weight of the Cavalier King Charles spaniel (Cross et al. 2009). There is a relationship between this mismatch in skull and brain volume and the development of syringomyelia. Cavalier King Charles spaniels with early-onset syringomyelia have a larger volume of parenchyma within a smaller caudal cranial fossa compared to older Cavalier King Charles spaniels with Chiari-like malformation only (Driver et al. 2010a, b). This suggests that Chiari-like malformation with syringomyelia is characterised by shortened skull and a lack of coordinated growth of the brain and skull, with a comparatively oversized brain. Moreover, further investigation has shown that Cavalier King Charles spaniels have relatively increased cerebellar volume compared to other breeds and that increased cerebellar volume in Cavalier King Charles spaniels is linked to the development of syringomyelia (Shaw et al. 2012). In addition increased cerebellar volume in Cavalier King Charles spaniels is correlated with increased crowding of the cerebellum in the caudal part of the caudal cranial fossa (Shaw et al. 2012).
The caudal cranial fossa can be subdivided into three regions, according to their bony walls. The caudal region is bounded by the occipital bones, the middle region by the squamous portion of the temporal bone and the rostral region by the tentorium cerebelli. Cavaliers have a strong relationship between hindbrain volume and rostral part of the caudal cranial fossa volume and a weak relationship between hindbrain volume and caudal part of the caudal cranial fossa volume. In Labrador retrievers and other small breed dogs, this relationship is reversed. This suggests that small breed dogs and Labrador retrievers compensate for variations in hindbrain volume by modifying the growth of the occipital skull. However, in the Cavalier King Charles spaniel, increased cerebellar size is not accommodated by increased occipital bone development and consequently the tentorium cerebelli compensates by bulging in a rostral direction (Shaw et al. 2013). In Cavalier King Charles spaniels with syringomyelia, the angle of the tentorium cerebelli is larger (Carrera et al. 2009). Increase in the angle of the tentorium is also reported in humans with Chiari-like malformation I (Sekula et al. 2005). The overcrowding in the caudal part of the caudal cranial fossa alters cerebrospinal fluid (CSF) dynamics. A phase-contrast cine MRI study indicated that obstruction to CSF flow at the foramen magnum is common in Cavalier King Charles spaniels (Cerda-Gonzalez et al. 2009b). The presence and severity of syringomyelia were positively associated with turbulent flow and jet particularly at the level of the C2–C3 intervertebral disc space. A higher peak CSF flow velocity at the level of the foramen magnum, combined with a lower CSF flow velocity at the level of the C2–C3 intervertebral disc, predicts a higher likelihood of development of a syrinx (Cerda-Gonzalez et al. 2009b). Additionally, in Cavalier King Charles spaniels, ventricle dimensions are positively correlated with syrinx width, supporting the theory that the clinical manifestations of Chiari-like malformation are related to CSF disturbances (Driver et al. 2010a).
14.3 Clinical Signs
Prevalence of syringomyelia is very high in some breeds but not all dogs are symptomatic. In a questionnaire study of all 6-year-old Danish Cavalier King Charles spaniels, the prevalence of dogs expressing signs consistent with syringomyelia was found to be 15.4 % (personal communication in an email from Dr. Mette Berendt 24th November 2011 mbe@life.ku.dk). By contrast MRI of asymptomatic 6-year-old Cavalier King Charles spaniels found a syringomyelia prevalence of 70 % (Parker et al. 2011). The most important and consistent clinical sign of Chiari-like malformation with syringomyelia is neuropathic pain , arising from damage and dysfunction of the central nervous system and disruption of the balance between nociceptive input and descending regulatory control from the brainstem. Owners may present dogs with signs of spinal pain and may describe spontaneous vocalisation, especially when the dog stands up, jumps or when it is picked up. Sleeping with the head in unusual positions and/or disrupted sleep may be reported (Fig. 14.5). Neuropathic pain can also manifest as allodynia , i.e. signs of discomfort from a non-noxious stimulus, such as touch or wearing a collar, or presumed dysaesthesia, which in the dog can manifest as phantom scratching (Fig. 14.6) or occipital/facial/ear rubbing (Rusbridge and Jeffery 2008). Signs may be exacerbated by excitement and exercise; it is thought because of increased systolic pulse pressure.
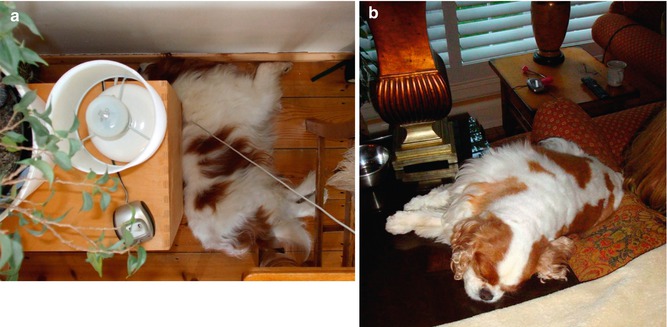

Fig. 14.5
(a) Cavalier King Charles spaniel with Chiari-like malformationand syringomyelia This dog routinely slept with his head dorsiflexed and wedged behind a solid object (Picture courtesy of Ms P Persson). (b) Cavalier King Charles spaniel with Chiari-like malformation and syringomyelia. This dog slept with her hindquarters lower than her head and with her head on a cooler surface. To achieve this, her head is on a wooden table and her hindquarters are balanced on a cushion and the back of a sofa (Picture courtesy of Mrs S Smith)
Fig. 14.6
‘Phantom scratching ’ in a Cavalier King Charles spaniel. This is typically unilateral and to the neck and shoulder region. Here the scratching left hind limb can be seen as a blur (arrow). The dog does not make skin contact. This behaviour can be elicited or exacerbated by excitement, exercise, touch and wearing of neck collars and harnesses (Picture courtesy of Ms J Harrison, Passionate Productions)
Pain is positively correlated with syrinx transverse width and symmetry on the vertical axis, i.e. dogs with a wider asymmetrical syrinx are more likely to experience discomfort, and dogs with a narrow symmetrical syrinx may be asymptomatic (Fig. 14.7) (Rusbridge et al. 2007). However, some dogs with Chiari-like malformation alone express signs of pain; for example, ear/back of skull rubbing, with vocalisation. Histopathological studies of syringomyelia in Cavalier King Charles spaniels found that dogs that expressed signs of pain had an asymmetrical syrinx, with profound alteration of dorsal horn laminar structure (Fig. 14.8) and reduced expression of pain-related neuropeptide substance P and calcitonin gene-related peptide (Hu et al. 2011a). Glial and fibrous proliferation was also associated with expression of clinical signs (Hu et al. 2011b). In symptomatic dogs the syrinx cavity margin is defined by a layer of condensed collagenous tissue, together with small blood vessels with abundant surrounding collagen (Fig. 14.9). Proliferative astrocytes (glial scar ) adjacent to the cavity are common. In contrast, the histopathological appearance for asymptomatic Cavalier King Charles spaniels is characterised by focal spongiosis, rarefaction and oedema, giving the neural tissue adjacent to the cavity a spongy appearance (Hu et al. 2011b).
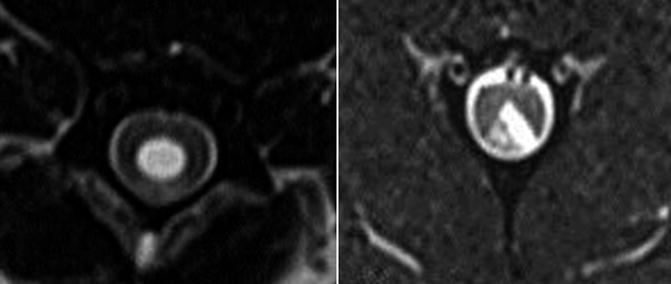
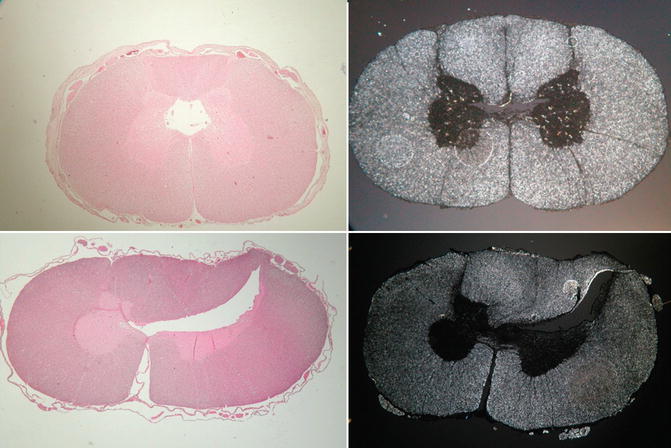
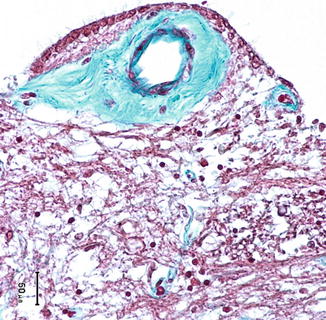
Fig. 14.7
Axial T2W images of the cervical spinal cord from dogs with asymptomatic (left) and symptomatic (right) syringomyelia. The syrinx in the symptomatic dog is asymmetrical and involves the spinal cord dorsal horn area. NB images are orientated according to the ‘human’ not the veterinary convention
Fig. 14.8
Dark field (left) and haematoxylin and eosin (right) histopathology sections of cervical spinal cord from Cavalier King Charles spaniels with asymptomatic (top) and symptomatic (bottom) syringomyelia. The syrinx in the symptomatic dog is asymmetrical, and loss of grey matter from the dorsal horn is evidence. In both dogs the central canal ependyma is lost (Picture courtesy of Drs Hilary Hu and Fernando Constantino-Casas)
Fig. 14.9
Histopathology sections of cervical spinal cord stained with Masson’s Trichrome stain from a symptomatic Cavalier King Charles spaniel with syringomyelia. In close proximity to the syrinx cavity, there are often an increased large number of small blood vessels, both arterial and venous suggestive of angiogenesis. These vessels are often surrounded by a copious amount of collagenous material with markedly thickened tunica media (suggestive of hypertrophy) (Picture courtesy of Drs Hilary Hu and Fernando Constantino-Casas)
Neuropathic pain has an important impact on an individual’s quality of life and neurobehaviour (Gustorff et al. 2008), and a recent study in syringomyelia-affected Cavalier King Charles spaniels found an association between the degree of neuropathic pain and fear-/anxiety-related behavioural changes (Rutherford et al. 2012). Dogs with higher neuropathic pain scores were more likely to act fearfully when approached by an unfamiliar person (stranger-directed fear), when in unfamiliar situations or when sudden loud noises occurred, e.g. thunderstorms (nonsocial fear). Dogs were more attached (‘clingy’) to the owners (attachment behaviour) and appeared to be more ‘afraid’ when left alone (separation-related behaviour). Additionally, dogs increased their attention-seeking behaviour and were more excitable in positive, reward-associated situations (excitability) (Rutherford et al. 2012). Cavalier King Charles spaniels with higher neuropathic pain score also showed decreased willingness to exercise and were more likely to have disturbed sleep (Rutherford et al. 2012).
Dogs with a wide syrinx and dorsal grey column damage are also more likely to have cervical torticollis and cervicothoracic scoliosis (Fig. 14.10). This is thought to be due to asymmetrical damage of the dorsal grey column, over a number of spinal cord segments, resulting in an imbalance of afferent proprioceptive information from the cervical neuromuscular spindles (Rusbridge et al. 2007; Van Biervliet et al. 2004). Syringomyelia may result in other neurological deficits, such as thoracic limb weakness and muscle atrophy (due to ventral horn cell damage) and pelvic limb ataxia and weakness (due to white matter damage or involvement of the lumbar spinal cord by the syrinx) (Rusbridge et al. 2006). Cavalier King Charles spaniels with Chiari-like malformation only, or Chiari-like malformation with syringomyelia, may also have subtle gait abnormalities, relating to cerebellar or spinocerebellar tract dysfunction. Investigation is ongoing to establish if these are acquired, for example, secondary to compression, or if they represent a developmental cerebellar abnormality (personal communication in an email from Dr. Holger Volk 26th June 2012 hvolk@rvc.ac.uk).

Fig. 14.10
A 2-year-old female Cavalier King Charles spaniel with cervicothoracic scoliosis and torticollis as a consequence of syringomyelia
There is a high incidence of epilepsy in dogs with Chiari-like malformation, especially in Cavaliers King Charles spaniels. In one report, 32 % of the study population had seizures (Lu et al. 2003), and in a long-term study of 48 Cavalier King Charles spaniels, with syringomyelia-associated neuropathic pain and where dogs with a history of seizures had been excluded from the original cohort, 12.5 % of the study population developed epilepsy in the follow-up period (Plessas et al. 2012). Consequently it has been suggested that there may be an association between Chiari-like malformation and epilepsy in the dog. An association has also been suggested in humans, but again it is unclear whether the association is coincidental (Granata and Valentini 2011). It is important to exclude the possibility of ‘drop attacks’, i.e. paroxysmal attacks of collapse, with or without loss of consciousness, abnormal extensor posturing and varying degrees of respiratory compromise, that are commonly associated with structural lesions of the cerebellum (Granata and Valentini 2011). In the Cavalier King Charles spaniel, it is also important to exclude the possibility of episodic collapse2 (Forman et al. 2012). A recent study compared ventricle size and caudal cranial fossa overcrowding and found no significant difference between Cavalier King Charles spaniels with Chiari-like malformation and seizures and those with Chiari-like malformation and other clinical signs but not seizures (Driver et al. 2013). Electroencephalogram evaluation, performed in three epileptic dogs, suggested paroxysmal abnormalities were mainly located over the frontal and temporal regions. Similar changes have been reported in humans with seizures and Chiari type I malformation (Elia et al. 1999). Further study is required to investigate if there is a connection between Chiari-like malformation and epilepsy. Vestibular dysfunction , facial nerve paralysis and deafness may also be seen, but, as with epilepsy, no direct relationship has been proven and this association may also be circumstantial.
14.4 Surgical Management
Medical and surgical treatment options exist for dogs with Chiari-like malformation with syringomyelia, and a possible approach to management is illustrated in Fig. 14.11. The main treatment objective is pain relief. The most common surgical management is craniocervical decompression, establishing a CSF pathway via the removal of part of the supraoccipital bone and dorsal arch of C1 (Vermeersch et al. 2004; Rusbridge 2007). Depending on the surgeon, this may be combined with a durotomy, with or without patching with a suitable graft material and with or without a cranioplasty, using titanium mesh or other prosthesis (Dewey et al. 2005, 2007). Craniocervical decompression surgery is successful in reducing pain and improving neurological deficits in approximately 80 % of cases, and approximately 45 % of cases may have a satisfactory quality of life 2 years post-operatively. However, surgery may not adequately address the factors leading to syringomyelia, and the syrinx appears persistent in the majority of cases (Dewey et al. 2005, 2007; Rusbridge 2007; Vermeersch et al. 2004). The clinical improvement is probably attributable to improvement in CSF flow through the foramen magnum. A syringosubarachnoid shunting procedure using a five French equine ocular lavage catheter has also been described. Clinical improvement in approximately 80 % of cases was reported, but there was no evidence of long-term syrinx resolution on post-operative MRI and dogs still expressed signs of neuropathic pain post-operatively (Motta and Skerritt 2012).
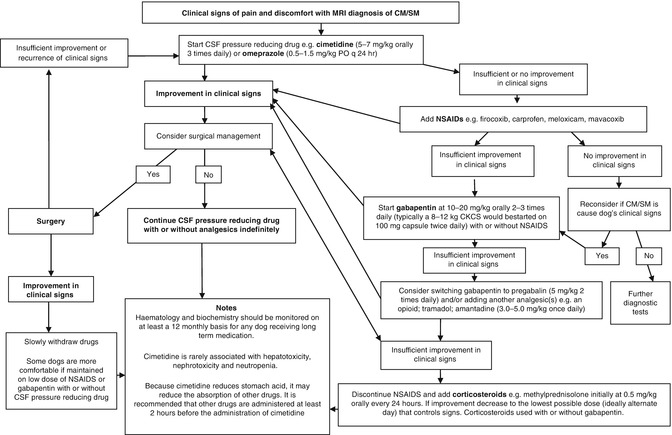
Fig. 14.11
Treatment algorithm for Chiari-like malformation and syringomyelia
14.5 Medical Management
Due to the persistence of syringomyelia and/or spinal cord dorsal horn damage, it is likely that the post-operative patient will require continuing medical management for pain relief. Also, in the majority of canine patients, medical management alone is chosen for financial reasons or owner preference. There are three main drugs used for treatment of Chiari-like malformation with syringomyelia: drugs that reduce CSF production (cimetidine or omeprazole ), analgesics (nonsteroidal anti-inflammatory drugs and antiepileptic drugs that have analgesic properties), and corticosteroids. As yet there are no scientific studies to prove the efficacy of these drugs in the management of neuropathic pain in dogs, and recommended management is based on anecdotal evidence only.
14.5.1 Drugs Reducing Cerebrospinal Fluid Production
In experimental models and using a ventriculocisternal perfusion technique, omeprazole reduces canine CSF production by 26 % (Javaheri et al. 1997). Although omeprazole is a specific inhibitor of H(+)-K(+)-activated ATPase, it is not clear if this is the mechanism by which it reduces CSF production (Lindvall-Axelsson et al. 1992). Cimetidine has been shown to be superior to ranitidine to reducing CSF production in an experimental cat model. The mechanism of action is proposed to be competitive inhibition of the histamine effect on H2 receptors located on the choroid plexus epithelial cell or by a direct effect on the capillaries of the choroid plexus (Naveh et al. 1992). However, there is also evidence that histamine may act physiologically by increasing the electrical activity of vasopressin-secreting neurons (Armstrong and Sladek 1985). Vasopressin reduces blood flow to the choroid plexus, thereby decreasing CSF production (Faraci et al. 1990). The usefulness of omeprazole or cimetidine on Chiari-like malformation, with or without syringomyelia, is unclear. It is often prescribed in the hope that this may limit disease progression, a variable that is difficult to assess in a scientific study of clinical cases. Some owners report a significant improvement in clinical signs of pain (Fig. 14.12). Adverse effects from these drugs are infrequently reported. Cimetidine retards P450 oxidative hepatic metabolism so caution is advised if using this preparation concurrently with other drugs metabolised by the liver, and with both cimetidine and omeprazole, periodic monitoring of haematology and serum biochemistry is advised. Absorption of gabapentin may be reduced with concurrent cimetidine administration so it has been advised that gabapentin is given 2 h before the cimetidine. An untried alternative may be gabapentin enacarbil, which is a prodrug of gabapentin, stable in gastrointestinal contents and absorbed throughout the intestinal tract by high-capacity nutrient transporters (Lal et al. 2010). It has been suggested that chronic hypergastrinaemia, caused by omeprazole, may increase the risk of gastric carcinomas, at least in laboratory rodent models, but this has not been reported in any other species (Hagiwara et al. 2011; Chapman et al. 2011).
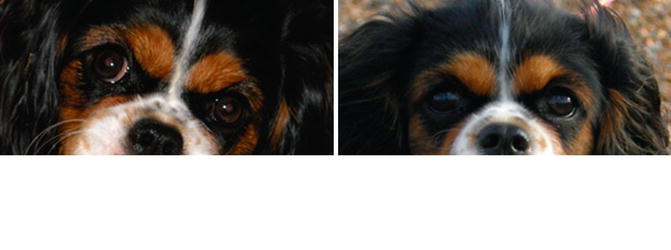
Fig. 14.12
A 2-year-old female Cavalier King Charles spaniel before (left) and after (right) medication with cimetidine. The image on the left shows ‘pain face’, i.e. a grimace suggesting discomfort. In contrast the dog’s expression on the right is more relaxed (Picture courtesy of Ms T Ledger)
Use of diuretics such as acetazolamide and furosemide for management of Chiari-like malformation and syringomyelia has also been described (Rusbridge et al. 2000; Rusbridge and Jeffery 2008). The use of acetazolamide is often limited by adverse effects, including lethargy, abdominal pain and bone marrow suppression (Rusbridge et al. 2000). Furosemide may not be ideal in toy breed dogs that also have a high likelihood of mitral valve disease (Lewis et al. 2011) and where the most common cause of death is congestive heart failure (Adams et al. 2010). Furosemide can result in significant increase in plasma aldosterone concentration and renin activity in healthy dogs (Pedersen 1996). This early activation of the renin-angiotensin-aldosterone system might be deleterious in an animal predisposed to heart disease (Connell et al. 2008). Moreover, long-term use of diuretics can lead to a diuretic-resistant state, which necessitates the use of higher doses, further activating the renin-angiotensin-aldosterone system (Parrinello et al. 2011).
14.5.2 Analgesics
Anecdotally, nonsteroidal anti-inflammatory drugs (NSAID S), e.g. meloxicam, carprofen, firocoxib and mavacoxib, can be useful in management of Chiari-like malformation and syringomyelia. NSAIDS are inhibitors of Cyclooxygenase-1 and/or Cyclooxygenase-2 and suppress inflammatory pain by reducing generation of prostanoids, in particular prostaglandin E2. Prostaglandin E2 also contributes to the genesis of neuropathic pain (Kawabata 2011). However, monotherapy with NSAIDs is unlikely to provide sufficient analgesia, especially if there has been damage to the spinal cord dorsal column. Therefore, in these situations, the addition of antiepileptic drugs with an anti-allodynic effect is recommended (Rusbridge and Jeffery 2008). Gabapentin and pregabalin modulate voltage-gated calcium channels resulting in a reduction of glutamate and substance P release and can be effective for neuropathic pain syndromes (Tremont-Lukats et al. 2000). Anecdotally, pregabalin is most efficacious for treating Chiari-like malformation and syringomyelia in dogs, but gabapentin can also be useful and is more economic. In severe cases that still have clinical signs, despite polypharmacy, the addition of opioids , tramadol or amantadine can be useful. It should be borne in mind that, with the exception of NSAIDs, there are no licenced oral analgesics in veterinary medicine.
14.5.3 Corticosteroids
Corticosteroids are believed to provide long-term pain relief because of their ability to inhibit the production of phospholipase-A-2 (Nolan 2000) and to inhibit the expression of multiple inflammatory genes coding for cytokines, enzymes, receptors and adhesion molecules (Barnes 1998). Corticosteroids are also reported to reduce sympathetically mediated pain (Gellman 2000) and decrease substance P expression (Wong and Tan 2002). Anecdotally, oral drugs such as methylprednisolone and prednisolone provide relief for some dogs with syringomyelia and can also be useful where there are significant neurological deficits, but adverse effects limit their usefulness for long-term therapy (Rusbridge et al. 2000).
14.6 Progression and Prognosis
The clinical signs of Chiari-like malformation and syringomyelia are often progressive. A recent long-term study, over a mean of 39 ± 14.3 months, found that approximately three-quarters of Cavalier King Charles spaniels with Chiari-like malformation and syringomyelia-associated neuropathic pain will deteriorate when managed medically, whereas one quarter remain static or improved (Plessas et al. 2012). However, despite this progression, all the owners of the alive dogs in this study reported that their dog’s quality of life was not severely compromised (Plessas et al. 2012). Fifteen percent of dogs were euthanased because of severe neuropathic pain. Morphometric values (volume of the caudal cranial fossa, parenchyma within the caudal cranial fossa and the sizes of the ventricles and syringes) were not correlated with prognosis. As discussed above, dogs with higher neuropathic pain scores are more likely to have fear-related behaviour, which can have a negative impact on the owner-perceived quality of life of a dog (Rutherford et al. 2012). Interestingly, obesity is also positively correlated with a reduced quality of life but not greater neuropathic pain. Obesity has an influence on the health and the quality of life in animals as it does in humans (German et al. 2012). In humans there is also a known association between increasing body mass index and CSF disorders such as idiopathic intracranial hypertension; however, it has not been established if the obesity is the cause or effect of this disease (Hannerz and Ericson 2009).
Some authors have suggested that early surgical intervention may improve prognosis, but robust studies evaluating this hypothesis have not been performed (Dewey et al. 2005). In addition, surgery does not necessarily improve long-term prognosis as 25–47 % of the operated dogs have recurrence or deterioration of the clinical signs within 0.2–3 years after surgery (Dewey et al. 2005, 2007; Rusbridge 2007). However, it should be remembered that it is probable that the groups of surgically managed cases contain dogs with more severe clinical signs so a valid comparison between medical and surgical management cannot be made at this time.
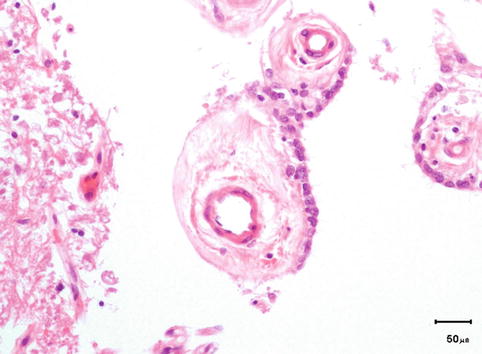
14.7 Learning About the Pathogenesis of Syringomyelia from Observations in Dogs
There are many poorly understood features of canine Chiari-like malformation and syringomyelia, including the pathogenesis of the syrinx and the precise origin of the pain. Pathological observations suggest that in the Cavalier King Charles spaniels, development of syringomyelia is related to increased central canal pressure. Central canal dilatation is typically the first change observed on MRI (Rusbridge et al. 2006), and disrupted integrity of the ependyma is a universal feature, regardless of clinical status (Hu et al. 2011b). Moreover there is an absence of pathological changes to suggest that fluid is drawn into the parenchyma from blood vessels or the subarachnoid space. For example, we do not see an accumulation of pools of fluid within the parenchyma, distant from the central canal. However, there is evidence of increased intra-canal pressure, in the form of tissue responses that would increase mechanical strength (Hu et al. 2011b). It has been demonstrated, in a contusion model of chronic spinal cord injury , that ascending central canal dilation occurs following injury and that expansion of the central canal lumen beyond a critical diameter corresponds with ependymal cell ciliary loss, together with thinning and a decrease in cell proliferation in the ependymal region.3 Normally, ependymal cells form a pseudostratified monolayer of epithelium that regulates fluid and electrolyte balance between the CSF and neuropil and also plays an important role in cellular signalling and wound repair in the spinal cord (Radojicic et al. 2007). In addition to ependymal disruption, pseudorosettes of ependymocytes may be observed, clustered around a core of fibrovascular tissue (Fig. 14.13), a finding also described by others (Williams and Weller 1973; Attar et al. 2005).