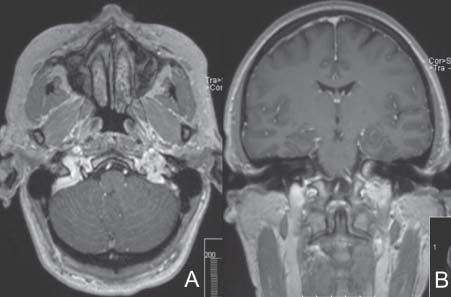
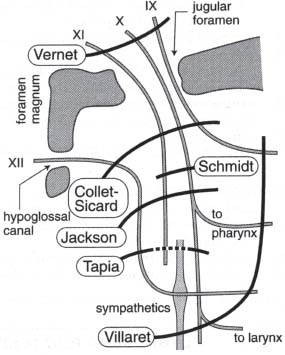
Case 25 Paraganglioma Fig. 25.1 T1-weighted magnetic resonance image with contrast injection. (A) Axial cut taken at the level of the skull base and (B) coronal cut. Fig. 25.2 Left external carotid artery injection angiogram. Fig. 25.3 Schematic diagram of jugular foramen syndromes. (From Greenberg MS. Handbook of Neurosurgery. 6th ed. New York: Thieme Medical Publishers; 2006:86. Adapted with permission.)
 Clinical Presentation
Clinical Presentation
 Questions
Questions

 Answers
Answers
< div class='tao-gold-member'>
25 Paraganglioma
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


