Case 33 Familial Cerebral Aneurysms
Hosam Al-Jehani and Richard Leblanc
Fig. 33.1 Pedigree demonstrating familial history of cerebral and peripheral aneurysms. (From Leblanc R. De novo formation of familial cerebral aneurysms. Neurosurgery 1999;44:871–877. Reprinted with permission.)
- A 24-year old white female was admitted to the hospital because of an episode of transient global amnesia, headache, nausea, and neck pain.
- The patient gave a family history of intracranial and peripheral aneurysms (Fig. 33.1),1 but the review of systems was unremarkable.
- She was normotensive and the remainder of the general and neurologic examinations were normal.
- A complete blood count, serum electrolytes, liver function tests, and urinalysis were normal. A chest x-ray, electrocardiogram, and ultrasound examination of the kidneys were unremarkable.
- A contrast-enhanced computed tomographic (CT) scan demonstrated a right internal carotid artery aneurysm, which was confirmed by four-vessel intraarterial cerebral angiography (Fig. 33.2).1 No other aneurysms were seen, but both posterior communicating arteries (PCOMs) had an infundibular origin.
- The patient underwent a right pterional craniotomy and uneventful clipping of the aneurysm.
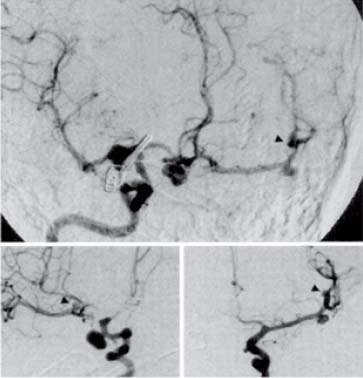
- The patient remained well until 10 years later when, at the age of 34 years, she was readmitted to the hospital because of severe headache. Cerebral angiography showed the presence of de novo aneurysms of the right internal carotid artery between the posterior communicating and anterior choroidal arteries, of the right middle cerebral artery at its bifurcation, of the anterior communicating artery, and on the left middle cerebral artery at the distal aspect of its first segment (M1) and at the bifurcation of its second segment (M2). The previously clipped aneurysm did not fill (Fig. 33.3).1
- The anterior communicating artery (ACOM) aneurysm was clipped, and the right internal carotid artery aneurysm was treated with detachable coils. The patient made an uneventful recovery. She was discharged home and returned to her previous occupation.
- The patient remained well for another 10 years when, at the age of 44 years, she underwent CT scanning for investigation of chronic, nonspecific facial pain. The CT scan showed that the previously untreated aneurysm of the second segment of the left middle cerebral artery had enlarged, a finding confirmed by intraarterial angiography. Angiography also demonstrated new aneurysms of the proximal and distal right middle cerebral artery, of the right ACOM and of the distal right superior cerebellar artery.
Fig. 33.2 Right carotid artery angiogram demonstrating the presence of a 1 × 1.5 cm aneurysm of the right internal carotid artery at the level of its bifurcation into anterior and middle cerebral arteries. (From Leblanc R. De novo formation of familial cerebral aneurysms. Neurosurgery 1999;44:871–877. Reprinted with permission.)
Fig. 33.3 Right internal carotid artery angiogram performed during compression of the left internal carotid artery (top) demonstrating the anterior communicating artery aneurysm and the aneurysms of the left middle cerebral artery at its bifurcation and at the origin of its second segment (arrowheads). The later two aneurysms are further illustrated at the bottom right image after the performance of a left internal carotid artery angiogram. The aneurysm at the origin of the right middle cerebral artery is illustrated at the bottom left of the figure. (From Leblanc R. De novo formation of familial cerebral aneurysms. Neurosurgery 1999; 44:871–877. Reprinted with permission.)
< div class='tao-gold-member'>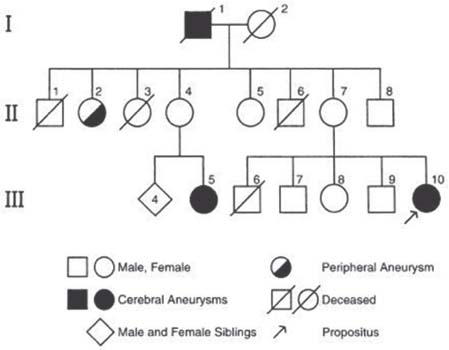
 Clinical Presentation
Clinical Presentation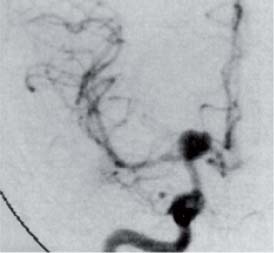
 Questions
Questions Answers
Answers


