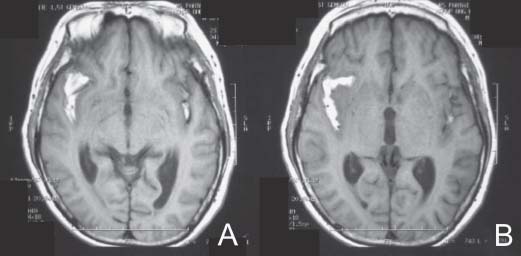
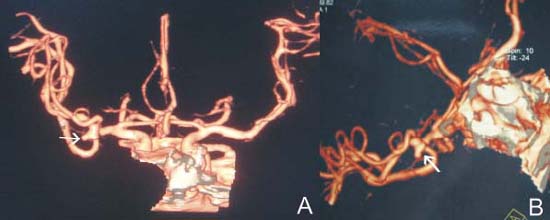
Case 36 Middle Cerebral Artery Aneurysm Fig. 36.1 T1- weighted magnetic resonance image without contrast performed on day 4 after patient’s severe headache revealing subarachnoid blood in the sylvian fissure seen in (A) and (B). Fig. 36.2 Computed tomography angiogram with three-dimensional reconstruction confirming the presence of a right middle cerebral artery aneurysm (arrow in [A] and [B]). The aneurysm has a “Mickey Mouse” appearance and originates from the bifurcation of right M1 segment of the middle cerebral artery.
 Clinical Presentation
Clinical Presentation
 Questions
Questions
 Answers
Answers
< div class='tao-gold-member'>
36 Middle Cerebral Artery Aneurysm
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


