Case 40 Moyamoya Disease
Abdulrahman J. Sabbagh, Jean-Pierre Farmer, Jie Ma, Ahmad I. Lary, and José Luis Montes
Fig. 40.1 Cerebral angiogram, internal carotid artery injection, with anteroposterior (A) and lateral (B) views.
- A 2-year-old girl had been born at term through a spontaneous vaginal delivery after a noneventful pregnancy.
- She was normal up to 14 months of age, when she presented with a left-sided simple partial motor seizure that was treated with an antiepileptic.
- At 23 months of age, she developed a new aphasia and right-sided weakness.
- Magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA) were performed, which prompted the ordering of an angiogram, shown in Fig. 40.1.
< div class='tao-gold-member'>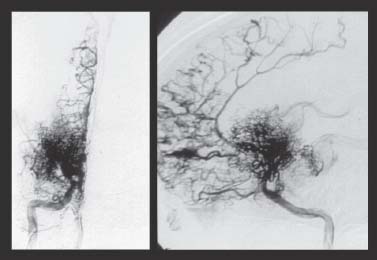
 Clinical Presentation
Clinical Presentation Questions
Questions Answers
Answers


