Figure 16-1 A lesion of the tibial nerve before its bifurcation into medial and lateral plantar divisions is seen on the noncontrast T1-weighted MRI image (arrow, right panel). The axial section corresponds to the T1 sagittal image provided for orientation (line, left panel). The mass features irregular margins and a plexiform component extending along the tibial nerve into its medial and lateral plantar divisions. These findings, although nondiagnostic, are consistent with a synovial sarcoma. A, anterior; P, posterior; L, left; R, right.
On exposure of the posterior tibial nerve, an obvious, well-encapsulated, 2.5- × 1.3-cm mass was found within its substance. On incision of the epineurium, the discrete, noninfiltrative tumor was easily resected from the nerve. Postoperatively, the patient’s symptoms improved significantly.
Histologic examination of the tumor demonstrated a demarcated, spindle cell neoplasm featuring intercellular collagen bands as well as focal glandular differentiation (Fig. 16-2). Immunohistochemistry showed the tumor to be variably reactive for keratin and epithelial membrane antigen (see Fig. 16-2). A histopathologic diagnosis of biphasic synovial sarcoma was made. The patient was referred for oncologic follow-up and underwent focal radiation therapy.
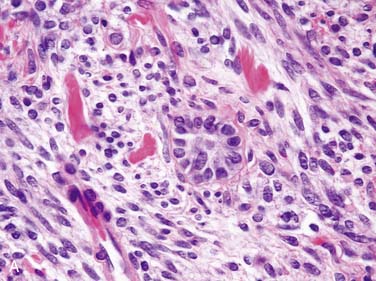
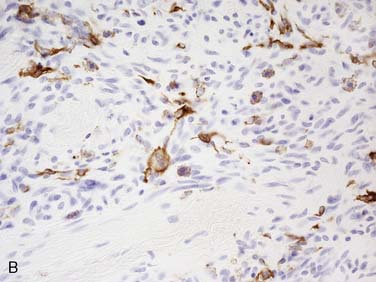
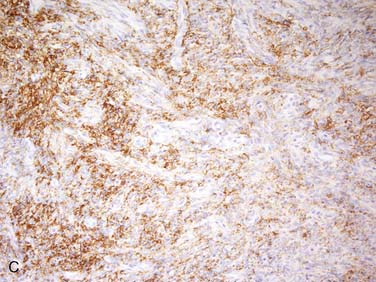
Figure 16-2 Microscopic sections of the tumor demonstrate a spindle cell tumor showing focal glandular differentiation (A), as well as variable keratin (B) and epithelial membrane antigen immunoreactivity (C).
CONCLUSIONS
Our understanding of the association between synovial sarcoma and the peripheral nervous system is limited to a handful of case reports. Involvement of peripheral nerve and nerve roots have been reported.2 Five of seven cases have shown biphasic histologic features. The majority of these tumors, five of seven cases, occurred in patients younger than 23 years of age. MRI findings usually consist of low to intermediate signal on T1 imaging and high signal on T2 imaging. The tumor often appears as a septated, inhomogeneous mass without clear margins. In up to 40% of synovial sarcomas, high signal on both T1 and T2 images can be seen related to intratumor hemorrhage.3
Synovial sarcomas have two basic histologic patterns, monophasic and biphasic. Biphasic synovial sarcomas are defined by a combination of spindle and epithelial cell components. Spindle cells are primarily uniform, plump cells with relatively sparse cytoplasm. The cells usually form densely cellular sheets and occasionally exhibit vague nuclear palisading. The epithelial component consists of cells with moderate amounts of pale cytoplasm and ovoid nuclei. Occasionally, these cells form true glands. Calcification is seen in up to 20% of tumors. Mast cells are also a prominent feature. Invariably, synovial sarcomas show immunoreactivity for cytokeratin and epithelial membrane antigen.4 Very useful in diagnosis, particularly in monophasic tumors, is the demonstration of a characteristic t(X;18 p11;q11) translocation, as shown by either fluorescence in situ hybridization or by polymerase chain reaction.5
The optimal treatment of synovial sarcoma consists of resection with wide margins, followed by adjuvant radiation therapy. The use of chemotherapy is debatable, and evidence for its efficacy is lacking.6 The 5-year survival rate varies from 36% to 76%.7 Predictors of a favorable prognosis include patient age less than 15 years, tumor size less than 5 cm, and occurrence of the tumor in distal portions of an extremity.8
Related posts:
 Malignant Peripheral Nerve Sheath Tumor
Disseminated Sporotrichosis with Multiple Granulomatous Mononeuropathies
Late Sporadic CMT4C—A New KIAA1985 Mutation
Late-Onset Transthyretin Val30Met Familial Amyloid Polyneuropathy Unrelated to Endemic Foci
A Case of Guillain-Barré Syndrome Associated with Anti-GD1b Immunoglobulin G Antibodies
Length-Related Axonal Loss in Neuropathy
Malignant Peripheral Nerve Sheath Tumor
Disseminated Sporotrichosis with Multiple Granulomatous Mononeuropathies
Late Sporadic CMT4C—A New KIAA1985 Mutation
Late-Onset Transthyretin Val30Met Familial Amyloid Polyneuropathy Unrelated to Endemic Foci
A Case of Guillain-Barré Syndrome Associated with Anti-GD1b Immunoglobulin G Antibodies
Length-Related Axonal Loss in Neuropathy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


