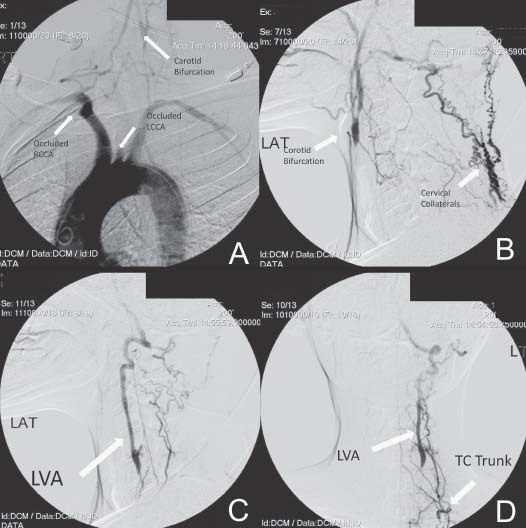
Case 43 Vertebral Artery Stenosis with Ischemia Fig. 43.1 Angiogram demonstrating the aortic arch and takeoffof the carotid, subclavian, and ver tebral ar teries. (A) More distal views demonstrating the left carotid bifurcation (B) and left vertebral artery (LVA) with collaterals (C) and (D). (TC, thyrocervical trunk.)
 Clinical Presentation
Clinical Presentation
 Questions
Questions
 Answers
Answers
< div class='tao-gold-member'>
43 Vertebral Artery Stenosis with Ischemia
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


