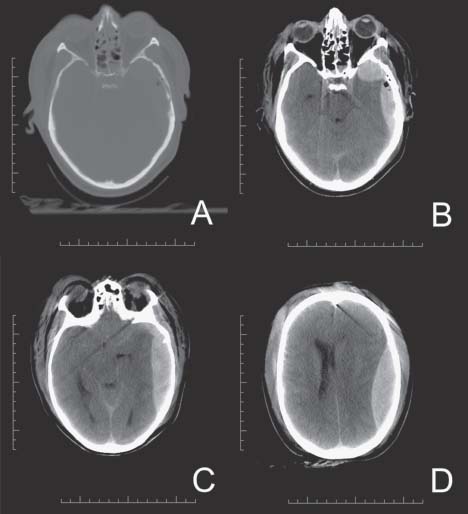
Case 47 Epidural Hematoma Fig. 47.1 Computed tomography scan of the head, bone window is displayed in (A) where a left temporal bone frac ture is seen. (B), (C) and (D) are brain windows showing a large epidural hematoma with significant mass effect and uncal herniation with brainstem compression and displacement (C) and significant midline shift (D).
 Clinical Presentation
Clinical Presentation
 Questions
Questions
 Answers
Answers
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue




