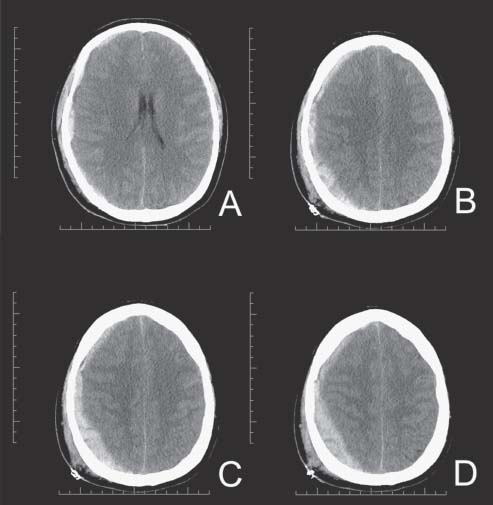
Case 48 Traumatic Acute Subdural Hematoma Fig. 48.1 Computed tomography scan of the head, brain windows showing a right-side subdural hematoma with associated midline shift greater than 5 mm (A) and brain compression (B–D).
 Clinical Presentation
Clinical Presentation
 Questions
Questions
 Answers
Answers
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue



