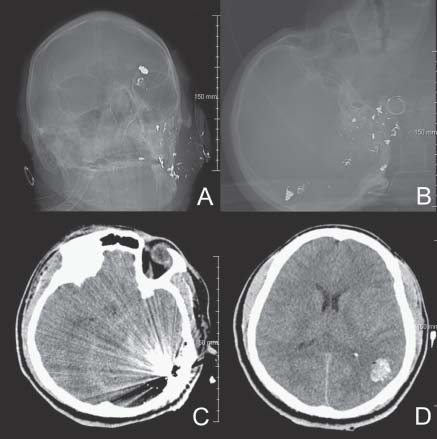
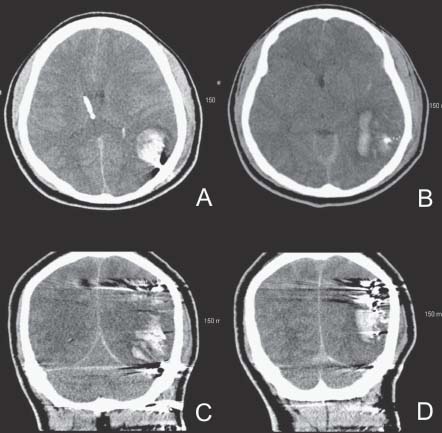
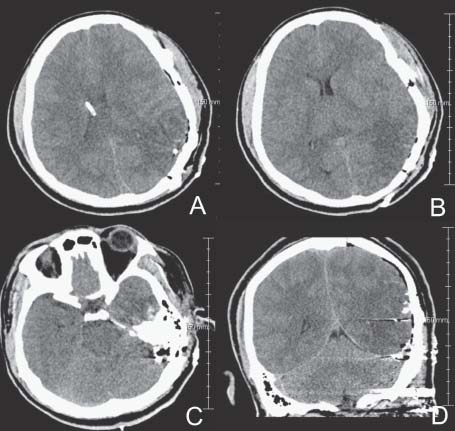
Case 51 Gunshot Wound to the Head Fig. 51.1 Computed tomography scan of the head. Scout images (A) anteroposterior and (B) lateral as well as pertinent axial images (C) and (D) are shown. The bullet entry site appears to be just under the left mastoid process and the bullet fragments appear to have traveled through the mastoid air cells and are lodged up into the left parietal lobe. Fig. 51.2 Computed tomography scan of the head show ing pertinent (A,B) axial and (C,D) coronal reconstructed images. See text for further details. Fig. 51.3 Computed tomography scan of the head showing pertinent (A–C) axial and (D) coronal reconstructed images. The hematoma has been evacuated. There is significant diff use brain edema, sulcal eff acement, tight basal cisterns, and small ventricles. These findings may be suggestive of increased intracranial pressure.
 Clinical Presentation
Clinical Presentation
 Questions
Questions
 Answers
Answers
< div class='tao-gold-member'>
51 Gunshot Wound to the Head
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


