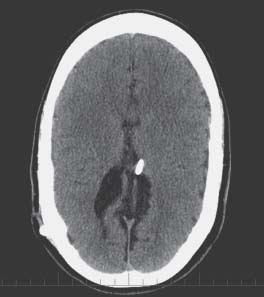
Case 55 Slit Ventricle Syndrome Fig. 55.1 Computed tomography scan of the brain revealing relatively small lateral ventricles and ventriculoperitoneal shunt located within the ventricle.
 Clinical Presentation
Clinical Presentation
 Questions
Questions
 Answers
Answers
< div class='tao-gold-member'>
55 Slit Ventricle Syndrome
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


