Case 56 Mega-hydrocephalus
Maqsood Ahmad and Abdulrahman J. Sabbagh
- You are called to see a newborn in the neonatal intensive care unit diagnosed prenatally with severe hydrocephalus.
- The patient was delivered at 38 weeks of gestation through an elective cesarean section with normal APGAR (appearance, pulse, grimace, activity, respiration) scores.
- On exam he has a head circumference that is 4 cm above the 97 th percentile, bulging fontanel, and splayed sutures. Additionally, distended scalp veins were present.
- Neonatal reflexes were present and he is spontaneously moving all limbs.
- He had no signs of spinal dysraphism or any skin manifestation of syndromic features.
Fig. 56.1 Computed tomography scan, axial section through the 4th ventricle (A), and higher cuts (B) and (C).
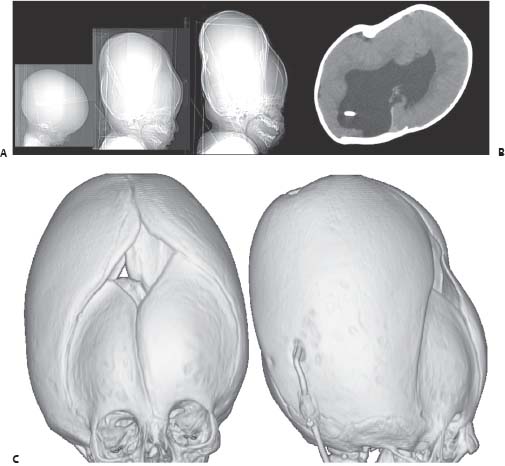
Fig. 56.2 Postshunting scout lateral images (A), axial computed tomography scan through the ventricles (B) and three-dimensional reconstructions of CT scan (C).
< div class='tao-gold-member'> Clinical Presentation
Clinical Presentation Questions
Questions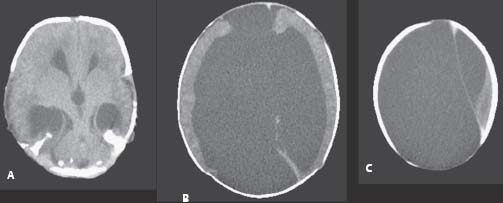
 Answers
Answers


