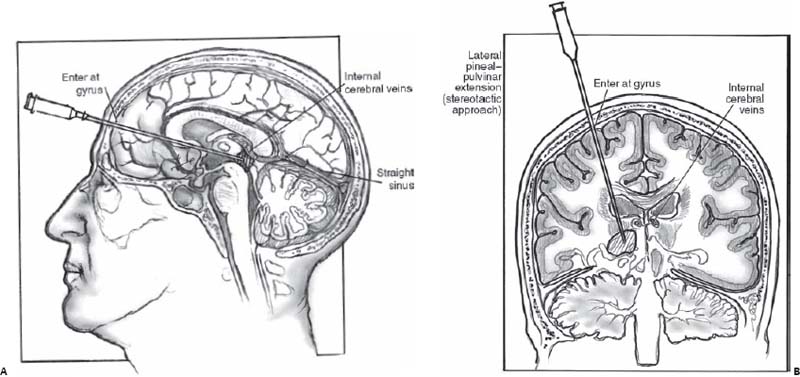
Case 60 Pineal Region Tumor Fig. 60.1 Computed tomography scan of the head without contrast at the level of the pineal gland. Fig. 60.2 Artist’s rendering of stereotactic approaches to pineal region tumors. (A) Low frontal (precoronal) approach avoids the internal cerebral veins above the tumor. (B) The lateral pineal pulvinar approach, which is lateral to the deep veins, is depicted. (From Sekhar L, Fessler R. Atlas of Neurosurgical Techniques: Brain. New York: Thieme Medical Publishers; 2006:570–571. Reprinted with permission.)

 Clinical Presentation
Clinical Presentation
 Questions
Questions
 Answers
Answers
< div class='tao-gold-member'>
60 Pineal Region Tumor
Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


