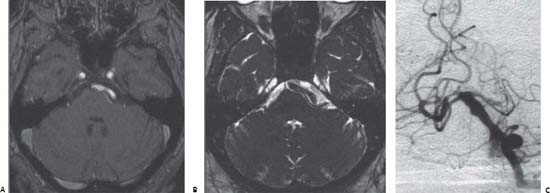
Case 74 Hemifacial Spasm and Microvascular Decompression Fig. 74.1 T2-weighted magnetic resonance image at the level of the posterior fossa. Fig. 74.2 (A) T1- and (B) T2-weighted magnetic resonance images at the level of the posterior fossa and cerebellopontine angle. (C) Vertebral digital subtraction angiography of the same patient.
 Clinical Presentation
Clinical Presentation

 Questions
Questions
 Answers
Answers
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue




