Sudden focal neurologic deficits can result from a variety of causes, the most frequent and concerning of which is acute stroke. The two most common forms of stroke that cause sudden onset of focal neurologic deficits without antecedent symptoms are acute ischemic stroke (AIS) and intracerebral hemorrhage (ICH). Both conditions are neurologic emergencies. The symptoms of AIS and ICH (Table 15.1) have significant overlap necessitating imaging studies to distinguish the two conditions.
The greatest opportunity to positively impact on the ultimate outcome of the patient with stroke occurs within the first hour of diagnosis and within 4 hours of the onset of symptoms. Emergency management of AIS is focused on attaining vascular reperfusion as soon as possible, most commonly with the administration of intravenous tissue plasminogen activator (IV tPA) for thrombolysis. In most cases, the outer limit of the time window for effective intervention is 4.5 hours after symptom onset. It has been estimated that every 15-minute reduction in onset-to-treatment time translates into a meaningful reduction in the risk of long-term disability at 3 months. In the case of ICH, emergency care is focused on blood pressure control, reversal of anticoagulation, and management of intracranial pressure (ICP).
This chapter focuses on the emergency management of the patient presenting with an acute focal neurologic deficit. Subsequent management after the first hour is discussed in Chapter 35 for AIS and in Chapter 38 for ICH.
PHASE 1: INITIAL MANAGEMENT AND IMAGING
Due to the importance of early intervention in stroke, the emphasis of emergency department (ED) management should not be on identifying subtle, unusual, or interesting neurologic signs but on the following five simple priorities. These tasks are ideally performed in parallel by four different personnel immediately upon patient arrival (e.g., the ED attending, resident, nurse, and stroke neurologist):
Assess level of consciousness and ensure adequate airway, breathing, and circulation.
Obtain the history with precise attention to the specific time of onset (or discovery) of symptoms along with a list of current medications.
Perform a National Institutes of Health (NIH) Stroke Scale examination.
Obtain head computed tomography (CT) imaging as soon as possible.
TABLE 15.1 Symptoms of Acute Stroke Symptoms of Acute Stroke
Facial asymmetry
Lateralized limb weakness or clumsiness
Lateralized numbness or paresthesias
Slurred or confused speech
Visual disturbances (diplopia or difficulty seeing)
Dizziness or vertigo
Gait instability
Headache
Alterations in level of consciousness
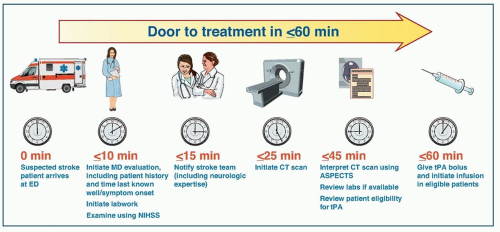
Modern emergency stroke management is evolving toward a paradigm that resembles trauma resuscitation. The initial goal is to minimize door-to-CT time because subsequent management is entirely dependent on the results of the scan. For AIS, the conventional goal is to obtain CT within 20 minutes and to start tPA infusion within 60 minutes of arrival to the ED (Figure 15.1). Currently, most hospitals struggle to have half of their AIS patients meet these targets.
New acute stroke care delivery models emphasizing parallel processing and lean management principles that exclude unnecessary steps have been shown to significantly reduce door-to-needle time for AIS. In the Helsinki model, physicians have proven the feasibility of safely administering IV tPA within 20 minutes of hospital arrival. In this paradigm, prehospital notification by ambulance triggers the stroke code, which then leads to the following:
Notification of the stroke team and ED staff, which assembles to meet the patient at the CT scanner
Transmitting the mobile phone number of any first responders or eyewitnesses to the stroke team to facilitate obtaining the history
Establishing a medical record number and hospital chart prior to arrival
Preordering the CT scan
Notification of pharmacy so that tPA or an anticoagulation reversing agent can be provided as soon as possible after CT
Given the complexity of coordinated personnel, resources, preparation, and teamwork that is required, most municipalities triage acute stroke patients directly to hospitals that are designated as primary stroke centers. After the initial resuscitation is completed, if the patient is unusually complex or critically ill, consideration should be given to transferring the patient to the nearest comprehensive stroke center.
INITIAL SURVEY AND VITAL SIGNS PRIOR TO COMPUTED TOMOGRAPHY
Level of Consciousness
ICH with mass effect as well as ischemic strokes of the brain stem, thalami, or large cortical regions can cause impairment in mental status. Depressed level of consciousness may in turn lead to aspiration of oropharyngeal contents or ineffective respirations due to upper airway obstruction, either of which may necessitate endotracheal intubation prior to further evaluation and management.
FIGURE 15.1 NINDS timeline targets for attaining an IV tPA door-to-needle time of 60 minutes or less. ED, emergency department; MD, doctor of medicine; NIHSS, National Institutes of Health Stroke Scale; CT, computed tomography; ASPECTS, Alberta Stroke Program Early CT Score; tPA, tissue plasminogen activator.
Blood Pressure
Hypertension occurs commonly as a nonspecific response to cerebral injury and can be present in both AIS and ICH. Elevated blood pressure (BP) is a strong indicator that the patient is actually having a stroke as opposed to a stroke mimic. Early BP elevation may be advantageous in AIS, allowing for increased cerebral perfusion to the ischemic penumbra, areas of marginally perfused brain. Aggressive BP reduction within the first few hours of AIS onset can lead to worsening of the neurologic deficit and therefore should be avoided.
BP should only be lowered prior to noncontrast CT if the systolic BP is higher than 220 mm Hg, diastolic BP is higher than 120 mm Hg [Level 1],1 or it is suspected that hypertension is leading to acute end-organ damage (e.g., acute myocardial infarction, aortic dissection, or cardiogenic pulmonary edema). If BP is lowered, a systolic BP of 180 mm Hg is the preferred target. The preferred agents and their dosages for emergency BP control in acute stroke are shown in Table 38.3. BP goals are reevaluated after CT imaging has established the etiology of the symptoms and, for AIS, once decisions are made regarding reperfusion therapy.
Heart Rate
Atrial fibrillation (AF) with rapid ventricular response (RVR) or other tachyarrhythmias can occur on presentation and may necessitate stabilization prior to obtaining CT. Diltiazem 10 mg IV or metoprolol 5 mg IV are commonly used initial therapies for AF with RVR in this setting. A cardiac monitor should be placed if there is any concern about heart rate or if the patient reports chest pain or palpitations. Routine electrocardiography should be obtained in acute stroke patients but is only required prior to CT if there is significant dysrhythmia or if an acute coronary syndrome is suspected.
Respirations and Breathing
Obvious respiratory distress should trigger placement of an oxygen saturation monitor and oxygen via nasal cannula. A decision whether to proceed directly to CT or to defer until adequate airway and ventilation can be assured then needs to be made. Patients with severe dyspnea or significantly impaired level of consciousness (stupor or coma) should be intubated prior to CT scan, as failure to control the airway can lead to respiratory arrest or severe aspiration.
Temperature
In general, it is not necessary to measure body temperature prior to CT in a patient with acute stroke unless meningitis is suspected.
INITIAL HISTORY
If eyewitnesses are available, obtain a collateral history from them to corroborate the patient’s account. Whenever possible, confirm the patient’s history with emergency medical system (EMS) personnel, and ask prehospital providers to provide mobile phone numbers of eyewitnesses who might not be immediately present in the ED. Be sure to inquire about the following points.
1. Exactly when did the stroke symptoms first begin?
If the onset of symptoms cannot be reported by the patient and were not witnessed, ask when the patient was last known well. For those who present on waking from sleep, the physician must determine whether the symptoms were present immediately upon awakening or shortly thereafter after a brief period of normalcy. If they truly awoke with the symptoms, the last known well time may be the time when they went to sleep the prior evening but often will be a time that they awoke transiently in the middle of the night.
2. What were the initial symptoms?
A maximal deficit at onset in a fully alert patient supports cerebral infarction and suggests embolism in particular. Ask specifically if the patient’s deficits have worsened or fluctuated since onset. Early headache, vomiting, or change in level of consciousness supports ICH. Inquire specifically about lateralized weakness, numbness, or other classic symptoms of acute stroke (see Table 15.1).
3. Was any seizure activity observed?
Postictal deficits from seizures can mimic stroke. Seizures manifesting as focal motor convulsions or generalized tonic-clonic activity can also occur at the onset of ICH or AIS, but this is unusual.
4. What is the patient’s medical history and neurologic baseline?
Assess for stroke risk factors such as hypertension, diabetes mellitus, dyslipidemia, cigarette smoking, AF, carotid stenosis, and prior transient ischemic attacks (TIAs) or strokes. A patient presenting with worsening of an existing or previously resolved neurologic deficit may have the “peeling-the-onion” syndrome (Table 15.2), with their symptoms resulting from unmasking of their prior deficit due to systemic derangements such as fever, hypoglycemia, or hypoxia.
5. What medications is the patient taking?
Ask particularly about anticoagulants or antiplatelet agents. Use of these agents not only predisposes to ICH but can also limit therapeutic options in the setting of ischemic stroke.
ESTABLISH INTRAVENOUS ACCESS AND DRAW ADMISSION LABS
Ideally, two peripheral IVs should be placed, at least one of which ideally should be 18 gauge to facilitate advanced imaging studies (i.e., CT angiography) if necessary. Labs should be drawn for complete blood count, serum chemistries, prothrombin time (PT)/partial thromboplastin time (PTT)/international normalized ratio (INR), troponin I, and other tests as indicated (e.g., liver function tests, toxicology screen, etc.). Point-of-care finger stick blood glucose level should also be obtained.
NATIONAL INSTITUTES OF HEALTH STROKE SCALE EXAMINATION
The National Institutes of Health Stroke Scale (NIHSS, Table 15.3) is a simple algorithm for quantifying the severity of neurologic deficits in patients with acute hemispheric or cerebellar syndromes. Eleven items are tested, and a score is generated on a scale ranging from 0 (no deficit) to 42 (comatose and quadriplegic). In expert hands, the test takes only several minutes to administer. When obtained within 6 hours of symptom onset, an NIHSS score greater than or equal to 7 indicates a nearly 85% chance of detecting a large-vessel intracranial occlusion by CT angiography. In hospitals that offer intra-arterial (IA) endovascular intervention for AIS, this cut point can be used to select patients for immediate CT angiography after the noncontrast CT has excluded blood in order to expedite endovascular therapies. Scores higher than 20 in patients with AIS imply a high risk of large territory infarction and a very poor prognosis if reperfusion is not attained. Once the history and examination are completed, the lesion should be able to be localized clinically.
PERFORM NONCONTRAST COMPUTED TOMOGRAPHY IMAGING
Noncontrast CT is by far the most readily available test for differentiation of AIS and ICH and the only one that must absolutely be obtained prior to administering thrombolytic therapy for AIS. The ability to obtain timely CT scans is greatly improved by having the CT scanner located within the ED. To minimize any delays in treatment, the patient should ideally be taken directly from the ambulance to the CT scanner with coordinated evaluation and intervention performed just outside the CT suite or on the CT table.
Studies show that obtaining CT imaging is the rate-limiting step in acute stroke management, so optimization of door-to-CT times should be of high priority. The main differential diagnosis in acute stroke is infarction versus hemorrhage. All further management decisions will depend on making this distinction.
Analysis for Hemorrhage
Blood is hyperdense (bright) and easily identifiable on noncontrast helical computed tomography (NCHCT) (Fig. 15.2A). ICH appears as a discrete focus of blood that displaces the surrounding brain parenchyma. ICH volume, a strong predictor of 30-day mortality and functional outcome, can be quickly measured using the ABC/2 method (see Fig. 38.3). Two diameters (A + B), measured at right angles on the slice that corresponds to the epicenter of the hemorrhage, are measured in centimeters. The third diameter perpendicular to that plane (C) is measured by multiplying the number of slices on which the bleed is apparent by each slice thickness (usually 5 mm, expressed 0.5 cm). The product of these three diameters is divided by two as a simplification of the equation for the volume of an ellipsoid. Patients with ICH volumes of less than 30 mL have potential for a good prognosis and have a small risk of early deterioration, whereas those with ICH volumes between 30 and 70 mL are at higher risk for early deterioration due to mass effect. Patients with hemorrhages greater than 70 mL were traditionally considered to be uniformly lethal, although survival with reasonable recovery can be attained in this group with emergency surgery, most often hemicraniectomy.
Whenever ICH is present, be sure to check for the following radiographic findings:
Subarachnoid hemorrhage (Fig. 15.2B) in association with intraparenchymal hemorrhage suggests a ruptured aneurysm and requires angiography.
Intraventricular hemorrhage (Fig. 15.2C) in association with ventricular enlargement requires neurosurgical evaluation for possible emergent ventriculostomy.
Fluid/fluid levels within a hematoma (Fig. 15.2D) result from separation of red blood cells and plasma and are indicative of a coagulopathy.
Edema, mass effect, and midline shift usually lead to delayed neurologic deterioration when associated with a large hemorrhage (> 30 mL). Perihematomal edema takes several hours to develop after ICH and is therefore not usually seen on initial head CT. An abnormally large or an irregular amount of edema associated with hemorrhage on initial presentation suggests (1) hemorrhagic conversion of infarcted tissue, (2) bleeding associated with neoplasm, or (3) venous infarction from dural sinus thrombosis.
Analysis for Ischemic Stroke
Infarction does not cause consistent changes on CT within 6 hours of stroke onset. Infarction is suspected when a patient presenting with sudden onset of neurologic deficits has a normal CT scan. Over a period of approximately 6 hours, regions of ischemia will gradually develop into an area of hypodensity as the tissue infarcts. The presence of a large hypodensity on NCHCT in an AIS patient should prompt reevaluation and careful scrutiny of the reported time of onset.
TABLE 15.2 Differential Diagnosis of Acute Neurologic Deficits
Diagnosis
Clinical Characteristics
Stroke
Ischemic stroke
Deficits that are maximal at onset suggest embolism
Sometimes preceded by transient ischemic attacks
Headache is uncommon
BP often elevated
Intracerebral hemorrhage
Often presents with headache and/or nausea and vomiting
Deficit commonly worsens over minutes to hours as hemorrhage expands
Loss of consciousness at onset is rare
BP often extremely elevated
Subarachnoid hemorrhage
Typically presents with sudden “thunderclap headache”
Often associated with transient loss of consciousness
Focal symptoms are unusual
Stroke Mimics
Seizure with postictal deficit
Occurs in aftermath of focal motor activity or an unwitnessed seizure
Deficits gradually improve and resolve over minutes to hours after onset
Can be differentiated from ischemic stroke with diffusion-weighted (DWI) MRI
EEG may show corresponding epileptiform activity
Migraine with aura
Typical patient has a history of migraine and prior similar events
Can present with weakness, aphasia, neglect, visual changes, and/or sensory loss
Symptoms may precede, be concurrent with, or follow a typical migraine headache
Typically occurs in younger women with no stroke risk factors
Unmasking of a prior focal deficit (i.e., “peeling-the-onion” phenomenon)
Sudden worsening of old stroke symptoms (does not cause new symptoms)
Triggered by fever, hypoxia, hypoglycemia, hyponatremia, or other metabolic disturbances
Focal deficits are typically accompanied by features of encephalopathy
Subdural hematoma
May not have a clear history of recent trauma in elderly patients with acute-on-chronic bleeding
Typically presents with focal deficits or subacute confusion and gait disturbance in an elderly patient
Headache is common but not universal
Brain tumor or abscess
Usually has a subacute to chronic presentation but can suddenly worsen due to associated seizure or bleeding into the tumor
Often with symptoms of headache, especially when recumbent
Multiple sclerosis or other demyelinating disease
Usually has a more subacute presentation but can mimic acute stroke at times
Often has history of prior deficits in varying locations
Can be differentiated from ischemic stroke with DWI MRI
Affects younger patients with no stroke risk factors
Peripheral (labyrinthine) vertigo
Can mimic an infarct in the brain stem or cerebellum causing acute vertigo
Can be differentiated from ischemic stroke with careful examination (horizontal head impulse test, characterization of nystagmus, and cover-uncover testa) in most but not all cases
Definitive exclusion of ischemic stroke requires DWI MRI, although DWI can also miss small brain stem infarcts
Most commonly presents with altered mental status, headache, vision changes, or seizures
Usually does not cause unilateral symptoms
BP usually elevated
Can occur in younger patients with no stroke risk factors
Conversion disorder
A diagnosis of exclusion
Detailed neurologic exam sometimes reveals inconsistencies suggesting a nonphysiologic cause of symptoms
Positive signs of misdirected effort may be elicited (e.g., Hoover sign)
BP, blood pressure; MRI, magnetic resonance imaging; EEG, electroencephalogram.
aSee Chapter 4 for details of the Head Impulse Nystagmus Test of Skew (HINTS) examination for differentiating central from peripheral vertigo.
TABLE 15.3 The National Institutes of Health Stroke Scale
1a. Level of consciousness (LOC):
0 =
Alert; keenly responsive
1 =
Not alert but arousable by minor stimulation to obey, answer, or respond
2 =
Not alert; requires repeated stimulation to attend or is obtunded and requires strong or painful stimulation to make movements (not stereotyped)
3 =
Responds only with reflex motor or autonomic effects or totally unresponsive, flaccid, and areflexic
1b. LOC questions: The patient is asked the month and his or her age.
0 =
Answers both questions correctly
1 =
Answers one question correctly
2 =
Answers neither question correctly
1c. LOC commands: The patient is asked to open and close the eyes and then to grip and release the nonparetic hand.
0 =
Performs both tasks correctly
1 =
Performs one task correctly
2 =
Performs neither task correctly
2. Best gaze: horizontal eye movements
0 =
Normal
1 =
Partial gaze palsy; gaze is abnormal in one or both eyes.
2 =
Forced deviation or total gaze paresis not overcome by the oculocephalic maneuver
3. Visual loss:
0 =
No visual loss
1 =
Partial hemianopia
2 =
Complete hemianopia
3 =
Bilateral hemianopia (blind including cortical blindness)
4. Facial palsy:
0 =
Normal symmetric movements
1 =
Minor paralysis (flattened nasolabial fold, asymmetry on smiling)
2 =
Partial paralysis (total or near-total paralysis of lower face)
3 =
Complete paralysis of one or both sides (absence of facial movement in the upper and lower face)
5. Motor arm: The limb is elevated for 10 s, scored separately for left and right.
0 =
No drift; limb holds 90 (or 45) degrees for full 10 s.
1 =
Drift; limb holds 90 (or 45) degrees but drifts down before full 10 s; does not hit bed or other support
2 =
Some effort against gravity; limb cannot get to or maintain (if cued) 90 (or 45) degrees, drifts down to bed, but has some effort against gravity.
3 =
No effort against gravity; limb falls.
4 =
No movement
6. Motor leg: The limb is elevated for 5 s, scored separately for left and right.
0 =
No drift; leg holds 30-degree position for full 5 s.
1 =
Drift; leg falls by the end of the 5-s period but does not hit bed.
2 =
Some effort against gravity; leg falls to bed by 5 s but has some effort against gravity.
3 =
No effort against gravity; leg falls to bed immediately.
4 =
No movement
7. Limb ataxia:
0 =
Absent
1 =
Present in one limb
2 =
Present in two limbs
8. Sensory:
0 =
Normal; no sensory loss
1 =
Mild to moderate sensory loss; patient feels pinprick is less sharp or is dull on the affected side; or there is a loss of superficial pain with pinprick, but patient is aware of being touched.
2 =
Severe to total sensory loss; patient is not aware of being touched in the face, arm, and leg.
9. Best language:
0 =
No aphasia; normal
1 =
Mild to moderate aphasia
2 =
Severe aphasia; all communication is through fragmentary expression.
3 =
Mute, global aphasia; no usable speech or auditory comprehension
10. Dysarthria:
0 =
Normal
1 =
Mild to moderate dysarthria; patient slurs at least some words and, at worst, can be understood with some difficulty.
2 =
Severe dysarthria; patient’s speech is so slurred as to be unintelligible in the absence of or out of proportion to aphasia.
11. Extinction and inattention:
0 =
No abnormality
1 =
Visual, tactile, auditory, spatial, or personal inattention or extinction to bilateral simultaneous stimulation in one of the sensory modalities
2 =
Profound hemi-inattention or extinction to more than one modality; does not recognize own hand or orients to only one side of space
Total score ranges from 0 (normal) to 42 (comatose and quadriplegic). For informational purpose only. Accurate and reliable scoring of the NIHSS requires strict adherence to a standardized testing protocol. Refer to www.ninds.nih.gov/doctors/NIH_Stroke_Scale.pdf for complete instructions on how to conduct and score the test and for smartphone applications than can assist in performance and scoring.
Only gold members can continue reading. Log In or Register to continue