8 CBF = cerebral perfusion pressure (CPP)/cerebrovascular resistance (CVR) CPP = systemic arterial blood pressure − intracranial pressure (ICP) exacerbates the damage produced by ischemia. In practice, many causes of stagnant or hypoxemic hypoxia (e.g. cardiac arrest and carbon monoxide poisoning, respectively) also depress cardiac output, resulting in combined hypoxic/global ischemic brain injury. Adult and infant brains react differently to hypoxia and ischemia. In general, infant brains are more resistant than those of adults; hypoxic-ischemic lesions have a different distribution in infants and adults reflecting an age-related differential (selective) vulnerability to such insults (Fig. 8.1). Because of the brain’s immense metabolic demands, after the onset of ischemia levels of brain glycogen, glucose, ATP and phosphocreatine plummet and are often depleted within 10 min of the acute event. After 15 min of cardiac arrest, up to 95% of the brain may be damaged. Primary respiratory arrest (e.g. due to aspiration, anaphylaxis, or airway trauma) may cause transient brain dysfunction, but less severe damage than ischemia. Optimal brain function and respiration are dependent upon the availability of glucose; however, the neuropathology of hypoglycemic brain injury differs from that due to hypoxia-ischemia. 8.1 Regions of selective vulnerability to hypoxic–ischemic damage are different in the adult and infant brain. Lesions may be considered as either acute/subacute or chronic. • severity and duration of insult • blood glucose level – high levels are associated with poor outcome • CNS (core) temperature – a lower temperature is protective. • 13% regained independent function during the first (post-arrest) year • initial presence of pupillary light reflexes, spontaneous eye movements, and extensor/flexor or withdrawal responses to pain were predictors of relatively good clinical outcome. APOPTOTIC: Apoptotic bodies/Nucleosomal segmentation The relative importance of apoptosis in AIE/HIE is debated; ultrastructural evidence suggests it is of minimal significance, though some apoptotic pathways may be activated in the course of necrotic cell death. Acute/subacute lesions include the following: 8.2 Coronal section through a nonperfused (‘respirator’) brain.
Adult hypoxic and ischemic lesions
TERMINOLOGY
Hypoxia
Global brain ischemia
 CELLULAR MECHANISMS OF ISCHEMIC CELL DEATH
CELLULAR MECHANISMS OF ISCHEMIC CELL DEATH
 Depolarization of neuronal/axonal membranes within 60–180 seconds of global anoxia leads to changes in extracellular and intracellular electrolyte composition and a decrease in ATP (secondary to impaired glycolysis and oxidative phosphorylation), with associated release of lactate and hydrogen ions and acidosis. ATP may decline to <25% of that in normally perfused tissue.
Depolarization of neuronal/axonal membranes within 60–180 seconds of global anoxia leads to changes in extracellular and intracellular electrolyte composition and a decrease in ATP (secondary to impaired glycolysis and oxidative phosphorylation), with associated release of lactate and hydrogen ions and acidosis. ATP may decline to <25% of that in normally perfused tissue.
 Cytoskeletal damage can affect the machinery of protein synthesis, but this may eventually recover.
Cytoskeletal damage can affect the machinery of protein synthesis, but this may eventually recover.
 Lipases, proteases and nucleases are activated, also with deleterious effects.
Lipases, proteases and nucleases are activated, also with deleterious effects.
 Free radicals and NO/peroxynitrite, a mediator of NO toxicity, increase.
Free radicals and NO/peroxynitrite, a mediator of NO toxicity, increase.
Local brain ischemia
PATHOPHYSIOLOGIC CONSIDERATIONS
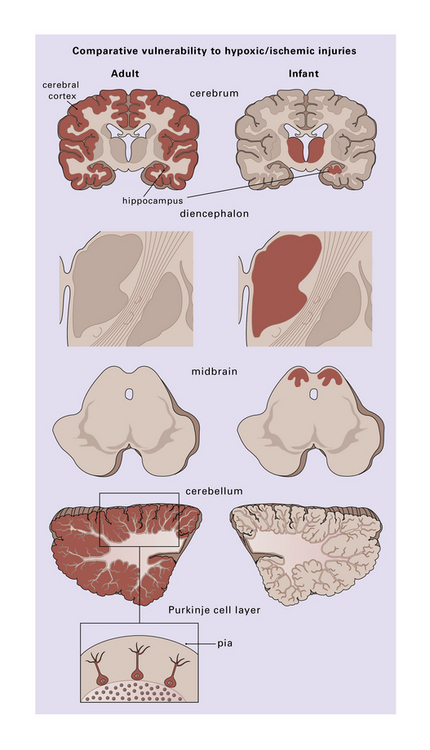
Those regions most susceptible to such an insult are colored in the diagram, though individual cases may show much significant variation. Inset (lower left) emphasizes the observation that cerebellar Purkinje cells are especially at risk during hypoxia.
PATHOLOGY
 Hypoxic-ischemic encephalopathy (HIE) has an extremely variable clinical presentation.
Hypoxic-ischemic encephalopathy (HIE) has an extremely variable clinical presentation.
 The severity and duration of HIE after transient cerebral hypoxia or ischemia depend upon:
The severity and duration of HIE after transient cerebral hypoxia or ischemia depend upon:
 In one study of many patients with HIE secondary to cardiac arrest:
In one study of many patients with HIE secondary to cardiac arrest:
 TYPES OF NEURONAL DEATH OF POTENTIAL IMPORTANCE IN HYPOXIC-ISCHEMIC DAMAGE
TYPES OF NEURONAL DEATH OF POTENTIAL IMPORTANCE IN HYPOXIC-ISCHEMIC DAMAGE
MACROSCOPIC APPEARANCES
 Precursors of cystic infarcts – especially in watershed territories.
Precursors of cystic infarcts – especially in watershed territories.
 Bright pink color and edema – after acute CO poisoning.
Bright pink color and edema – after acute CO poisoning.
 Generalized dusky discoloration and softening – the appearance of ‘non-perfused’ brain (Fig. 8.2).
Generalized dusky discoloration and softening – the appearance of ‘non-perfused’ brain (Fig. 8.2).
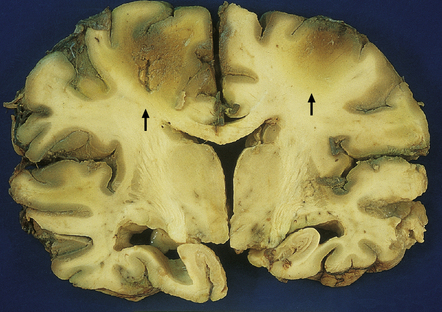
The brain is edematous with focally accentuated gray-brown discoloration throughout the cortex and extending into the subcortical white matter, most notably in the watershed regions (arrows) between the perfusion territories of the middle and anterior cerebral arteries.![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Adult hypoxic and ischemic lesions
 CEREBRAL BLOOD FLOW (CBF)
CEREBRAL BLOOD FLOW (CBF)









 ROLE OF ASTROCYTES
ROLE OF ASTROCYTES




 REPERFUSION AFTER CIRCULATORY ARREST
REPERFUSION AFTER CIRCULATORY ARREST



 HYPOXIC-ISCHEMIC BRAIN INJURY
HYPOXIC-ISCHEMIC BRAIN INJURY





Only gold members can continue reading. Log In or Register to continue


