Fig. 1.1
Anatomical picture showing the posterior wall of the sphenoid sinus; all the anatomical landmarks are visible, but they may vary according to the degree of pneumatization of the sphenoid sinus. ^ tuberculum sellae as seen from the endoscopic endonasal view (recently called the “suprasellar notch”), C clival indentation, CPc paraclival segment of the carotid protuberance, CPs parasellar segment of the carotid protuberance, ocr lateral optocarotid recess, OP optic protuberance, PS planum sphenoidale, SF sellar floor
Once the sellar dura is opened, the anterior lobe of the pituitary gland comes into view. Its inferior surface usually conforms to the shape of the sellar floor, but its lateral and superior margins vary in shape because these walls are composed of soft tissue rather than bone. Posteriorly, the neurohypophysis (posterior pituitary gland) can be observed and is often softer, gelatinous, and more densely adherent to the posterior sellar wall, the dorsum sellae. Above, the diaphragma sellae covers the pituitary gland, except for a small central opening through which the pituitary stalk (infundibulum) passes. Folds of dura mater, which constitute the lateral walls of the hypophyseal fossa, also comprise the medial wall of the cavernous sinuses; the internal carotid artery (ICA) coursing through the cavernous sinus can be appreciated at this level [11, 13].
The pituitary gland derives its blood supply from two major groups of arteries. The superior hypophyseal artery primarily supplies the anterior lobe, the pituitary stalk, and the inferior surface of the optic nerve and chiasm, whereas the inferior hypophyseal artery is primarily related to the pars nervosa. The superior hypophyseal artery can arise from the supraclinoid portion of the ICA or from the posterior communicating artery, whereas the inferior hypophyseal artery arises from the meningohypophyseal trunk, a branch of the cavernous segment of the ICA.
1.4 Extended Endoscopic Transsphenoidal Approaches
1.4.1 Suprasellar Area
The sphenoid sinus represents a window of access to the midline skull base via the endonasal corridor; when the sinus is well pneumatized, all main bony landmarks can be identified. The sellar floor occupies a central position, with the planum sphenoidale above and the clival indentation below; on both sides, lateral to the sellar floor, are the two bony prominences of the intracavernous internal carotid arteries, and the optic nerves can be identified slightly superiorly. Between these two protuberances, depending on the degree of pneumatization of the sphenoid sinus, the projection of the optic strut of the anterior clinoid process creates the lateral opticocarotid recess [7, 13–15].
Immediately above, the tuberculum sellae can be seen as an indentation represented by the angle formed by the convergence of the planum sphenoidale with the sellar floor. Recently, we renamed this structure as the “suprasellar notch” [16]. Anteriorly lies the planum sphenoidale, which is limited on both sides by the optic nerve protuberances, diverging toward the orbits.
The removal of the upper half of the sella, the tuberculum sellae, and the posterior portion of the planum sphenoidale offers the possibility of exploring and operating in the suprasellar region (Fig. 1.2). The entire suprasellar region can be divided into four intradural areas: the suprachiasmatic region, the subchiasmatic region, the retrosellar region, and the ventricular region [15].
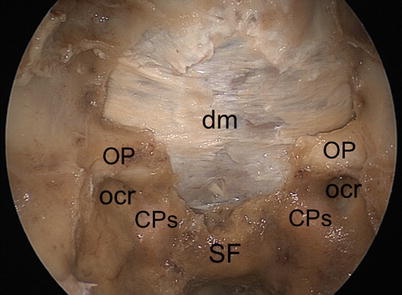
Fig. 1.2
The pattern of bony removal of the planum sphenoidale resembles a chef’s hat, limited in its posterior part by the medial border of the lateral optocarotid recess (ocr) and by the bony prominence of the optic nerve. CPc paraclival segment of the carotid protuberance, CPs parasellar segment of the carotid protuberance, dm dura mater of the planum sphenoidale, OP optic protuberance, SF sellar floor
In the suprachiasmatic region, the chiasmatic and the lamina terminalis cisterns are accessible. The anterior margin of the optic chiasm and the medial portion of the optic nerves, the anterior cerebral arteries, the anterior communicating artery, and the recurrent arteries of Heubner can be identified, together with the gyri recti of the frontal lobes [17].
In the subchiasmatic space, the pituitary stalk is encountered below the optic chiasm, with the superior hypophyseal arteries and their perforating branches supplying the inferior surface of the optic chiasm and the optic nerves (Fig. 1.3). The superior aspect of the pituitary gland and the dorsum sellae are also visible.
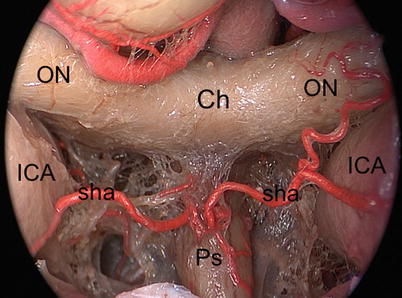
Fig. 1.3
Intradural exploration of the suprasellar area after removal of the tuberculum sellae and planum sphenoidale. Ch chiasm, ICA internal carotid artery, ON optic nerve, Ps pituitary stalk, sha superior hypophyseal artery
The retrosellar area, explored by passing with the endoscope between the pituitary stalk and the ICA above the dorsum sellae, includes the upper third of the basilar artery, the pons, the superior cerebellar arteries, the oculomotor nerves, the posterior cerebral arteries, the mammillary bodies, and the floor of the third ventricle [18, 19].
The third ventricle can be opened at the level of the tuber cinereum and the endoscope can be advanced into the ventricular cavity, obtaining a panoramic view of the ventricular area, including the thalami and the massa intermedia, the foramina of Monro and anterior commissure anteriorly, the choroid plexus of the third ventricle, the pineal and the suprapineal recesses, the posterior commissure, the habenular commissure, the habenular trigone, and the cerebral aqueduct posteriorly.
1.4.2 The Parasellar Area
The parasellar area is accessible through the lateral wall of the sphenoid sinus. The cavernous sinus apex and the trigeminal maxillary and mandibular nerve protuberances usually lie on its bony surface (Fig. 1.4). Once bone has been removed, the medial cavernous sinus wall (composed of fibrous trabecular tissue) is visualized, enclosing the C-shaped segment of the intracavernous internal carotid artery [20–23] (Fig. 1.5).
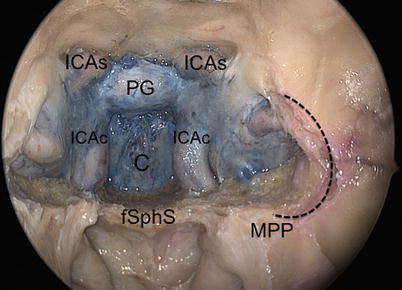
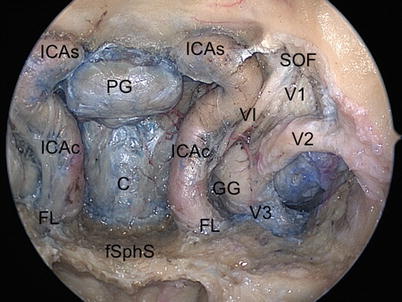
Fig. 1.4
Endoscopic view after bony removal of the sella, clivus (C), and the intracavernous internal carotid arteries. The medial pterygoid process has been drilled away, thus allowing a wide exposure of the lateral recess of the sphenoid sinus. The dotted line represents the lateral recess of the sphenoid sinus after drilling of the medial pterygoid process. ICAc paraclival segment of the internal carotid artery, ICAs parasellar segment of the internal carotid artery, fSphS floor of the sphenoid sinus, MPP medial pterygoid plate, PG pituitary gland
Fig. 1.5




Endoscopic view after bony removal of the lateral recess of the sphenoid sinus. C clivus, ICAc paraclival segment of the internal carotid artery, ICAs parasellar segment of the internal carotid artery, FL foramen lacerum, fSphS floor of the sphenoid sinus, GG Gasserian ganglion, PG pituitary gland, SOF superior orbital fissure, V1 first branch of trigeminal nerve, V2 second branch of trigeminal nerve, V3 third branch of trigeminal nerve, VI abducens nerve
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
